Cost-Effectiveness of Endovascular Intervention Versus Bypass Surgery in Patients With Chronic Limb-Threatening Ischemia and Principal Target Lesion in the Femoropopliteal Segment
Angelica Perlander, MD1; Joakim Nordanstig, MD, PhD1; Klas Österberg, MD, PhD1; Mikael Svensson, PhD2
ISSN: 2694-3026
J CRIT LIMB ISCHEM 2022;2(1):E19-E26. Epub 2022 February 7.
Abstract
Background. Chronic limb-threatening ischemia (CLTI) commonly requires revascularization to alleviate symptoms and prevent amputation. This study investigates the cost-effectiveness of bypass surgery vs endovascular intervention in CLTI with femoropopliteal lesions. Methods. Between March 2011 and January 2015, a total of 160 CLTI patients, undergoing bypass surgery (n = 55) or endovascular intervention (n = 105), were included in a prospective cohort study. The main study endpoint was quality-adjusted life years (QALYs) based on self-registered EQ-5D-3L questionnaires. Costs were retrieved from the hospital’s cost-per-patient system. The incremental cost-effectiveness ratio (ICER) was calculated as costs per gained QALY and per avoided amputation. Results. QALYs during 2 years of follow-up were 1.04 years (95% CI, 0.89-1.18) in the bypass group and 0.95 years (95% CI, 0.84-1.07) in the endovascular group, with no significant intergroup difference. Amputation-free survival was 78% in the bypass group and 59% in the endovascular group (P<.05). The mean total cost per patient was $42,900 (95% CI, 32,400-53,500) for bypass surgery and $22,200 (95% CI, 17,800-26,600) for endovascular treatment. The cost per gained QALY and per avoided amputation with bypass surgery vs endovascular intervention was $730,000 and $104,000, respectively. Conclusion. At 2 years, the mean total hospital cost post bypass surgery was almost twice the cost post endovascular intervention. Although amputation-free survival was higher after bypass surgery, there was no corresponding gain in generic health status. This led to a high additional cost per QALY gained and per amputation avoided with bypass surgery compared with endovascular intervention.
J CRIT LIMB ISCHEM 2022;2(1):E19-E26. Epub 2022 February 7.
Key words: bypass surgery, chronic limb-threatening ischemia, cost-effectiveness, endovascular intervention, quality-adjusted life years
Introduction
Chronic limb-threatening ischemia (CLTI) refers to the most severe stage of impaired arterial circulation in the lower extremities, most often due to atherosclerosis, resulting in ischemic rest pain, non-healing ulcers and/or gangrene. The impact of CLTI on health-care resources is considerable and it represents a growing burden in many countries, with an increasingly elderly population and a rising incidence of type 2 diabetes mellitus, which are 2 factors strongly associated with CLTI.1-3 Revascularization procedures to improve and maintain tissue perfusion are crucial for the alleviation of CLTI symptoms and to avoid major limb amputation.3-8 The superficial femoral artery and popliteal artery are the most common target segments for invasive treatment in CLTI.9,10 Regardless of revascularization method, repeat procedures are commonly needed to maintain patency, which may place additional burden and costs on health-care vascular services.2,11-13
Cost-effectiveness analyses of CLTI patients are scarce. It has been shown that an invasive treatment strategy is cost-effective compared with conservative treatment with local wound care or primary amputation.14-16 The only randomized controlled study that has compared the cost-effectiveness of different invasive treatment strategies in CLTI is the BASIL (Bypass versus Angioplasty in Severe Ischemia of the Leg) study.17 A small but insignificant health-outcome benefit was reported with bypass surgery compared with endovascular revascularization as first-line strategy, at the expense of a moderate cost increase. Since then, a limited number of studies have addressed the health economic issue of invasive treatment of CLTI. A clear majority are retrospective studies reporting a lower cost for endovascular intervention compared with open surgery.2,18-22 Notably, all of these studies, as well as a more recent prospective study,23 have included mixed patient populations with either claudication or CLTI, 2 patient groups with markedly different prognoses. This substantially limits the overall possibility to adequately relate costs to clinical outcomes.9 To our knowledge, only 2 cost-effectiveness studies on patients with exclusively CLTI have been published over the past 2 decades16,24 and only 1 study—a Markov model based on previously published data—related costs to patient-reported health measures.16 Overall, there have been few cost-effectiveness analyses on CLTI patients using generic measures of health gain, despite generally being considered the most relevant method in health-economic evaluations.25 Against this background, the aim of this study was to investigate the cost-effectiveness of bypass surgery vs endovascular treatment in CLTI patients undergoing revascularization in the femoropopliteal segment based on patient-reported health-related quality-of-life measures and prospectively collected granular patient-level cost data.
Methods
Study population. This study was based on a prospective observational cohort study performed at Sahlgrenska University Hospital in Gothenburg, Sweden. Between March 2011 and January 2015, a total of 160 patients presenting with CLTI and principal atherosclerotic target lesion in the superficial femoral artery or popliteal artery were included in the study. Choice of revascularization method was based on the Trans-Atlantic InterSociety Consensus (TASC) II treatment guidelines and the treatment decision was made by the vascular team, represented by both open surgical and endovascular expertise, at regular treatment conferences. Accordingly, TASC II A lesions were treated endovascularly and the majority of TASC II D lesions were treated with bypass surgery. In TASC II B and C lesions, the patient’s comorbidity and risk profile as well as lesion severity (degree of calcification, run-off situation) also influenced the treatment decision. All patients were subjected to the same surveillance program regardless of mode of revascularization: clinical follow-up by a vascular surgeon at 1, 12, and 24 months and duplex ultrasound at 1, 3, 7, and 12 months. Significant stenosis (>2.5-fold increase in peak flow velocity) led to reintervention irrespective of current symptomatology. The study was approved by the regional ethical review board of the University of Gothenburg (reference number 316-09), and has been registered in the ClinicalTrials.gov database (NCT01794494). All study participants provided written informed consent before entering the study.
Collection of generic health status data. Self-reported generic health status was assessed before revascularization and at each follow-up visit using the EuroQol 5 Dimensions instrument with 3 scale steps (EQ-5D-3L). EQ-5D is one of the most commonly used generic health-status classification systems in health-economic evaluations.26 EQ-5D-3L covers 5 dimensions of health, ie, mobility, self-care, ability to undertake usual activities, pain/discomfort, and anxiety/depression. Patients were asked to mark 1 of 3 levels (no problems, some problems, or severe problems) that corresponded most to their experience or function within each dimension. The Dolan tariff, a well-established prediction model, was used to calculate quality-adjusted life year (QALY) weights on the index scale 0 to 1, where 0 corresponds to a state of death and 1 corresponds to the best possible health state.27 QALYs were then calculated by multiplying the QALY weight with the time spent at each level of health state over the 2-year follow-up (linear interpolation between each measurement point). For patients who were amputated, the study protocol did not include any subsequent EQ-5D-3L reports. Therefore, for these patients, QALY weights after amputation were estimated based on data from the Swedish Amputation and Prosthesis Registry (QALY weight 0.51 for transfemoral amputations and 0.56 for transtibial amputations).28 These data refer to 5762 lower-limb amputations conducted in Sweden between 2011 and 2018, of which 85% were due to diabetes and/or vascular causes. QALY weights from this registry correspond well with those recommended based on other studies, for the purpose of cost-effectiveness analyses.3
Collection of cost data. Resource-use data were collected from the hospital’s cost-per-patient system, including costs for health-care staff, endovascular and surgical procedures, anesthetic procedures, postoperative care, radiologic diagnostic procedures, laboratory tests, and in-hospital use of drugs. Costs were collected for a time period of 2 years and 3 months from the index procedure to ensure that all follow-up visits over the 2 years fell within the observation window and were included in the overall analysis. All costs relating to both outpatient visits and hospital stays at the department of vascular surgery were registered. When patients were directly transferred to a geriatric ward after the vascular procedure, without hospital discharge, the cost for that hospital stay was also included. For patients who subsequently underwent a major limb amputation, costs for related hospital stays and outpatient visits at the orthopedic and rehabilitation clinics were also registered.
In 4 cases, cost data were missing or inadequate in the hospital’s cost database and those patients were excluded from analysis. In 6 cases, patients started or ended their hospital stay at another clinic due to concurrent disease or comorbidities not directly connected to the revascularization procedure. As registered costs comprised the entire in-hospital stay, an average cost per day was then calculated and allocated to the time spent in the vascular ward. In 2 cases, patients had similar repeated procedures (percutaneous transluminal angioplasty), but cost was missing for 1 event. An average cost for the other occasions in which cost data were available was then imputed. Finally, in 2 patients who underwent amputation, the hospital stay included other medical care (for example, radiotherapy due to a cancer diagnosis). An average cost for a hospital stay due to a major amputation within the study was then imputed.
Statistics. Descriptive statistics are presented as absolute numbers and relative frequencies. Student’s t test was used for variables with continuous data and Fisher’s exact test for discrete variables. Cost data are presented as mean values with 95% confidence intervals (CIs). Cost-effectiveness analysis was undertaken from a health-care payer perspective. All costs were converted from Swedish kronor to United States dollars (USD) at an exchange rate of 8.27 SEK per USD (exchange rate on January 1, 2021) and consequences in year 2 were discounted at an annual 3% discount rate. The average cost attributable to all aspects of the vascular care for the 2 treatment groups during the study period was calculated. A linear regression analysis was performed to adjust for differences in demographic and comorbidity status between study arms. The incremental cost-effectiveness ratio (ICER) was calculated by dividing the difference in mean costs between groups with the difference in mean QALYs and by the difference in amputation rate. Sampling uncertainty was addressed using non-parametric bootstrapping with 1000 bootstrap resamples and results are presented with the bootstrapped 95% CIs. Statistical significance was assumed at P<.05. Statistical analysis was performed using SPSS, version 22 (IBM Corporation) and Stata, version 16.
Results
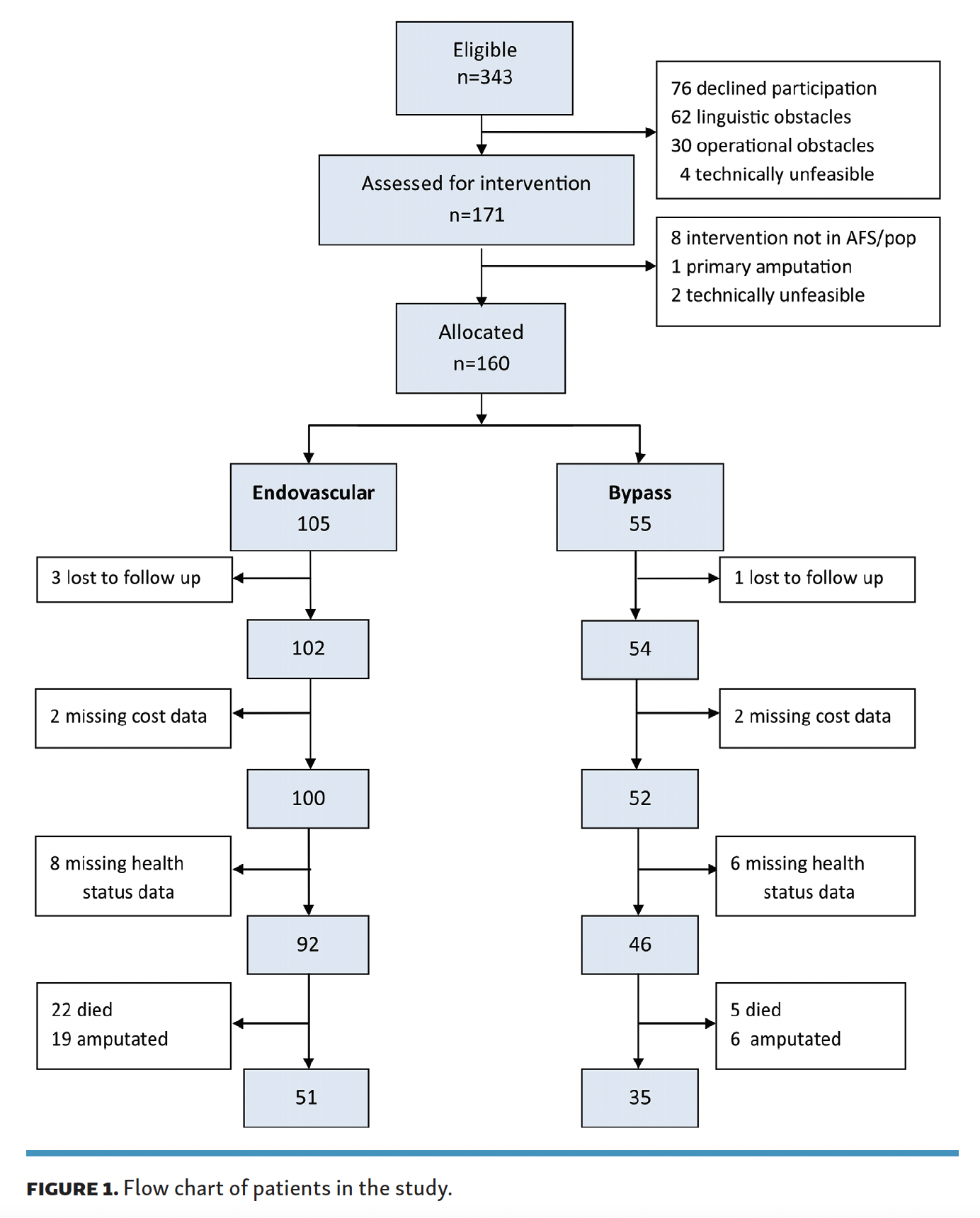
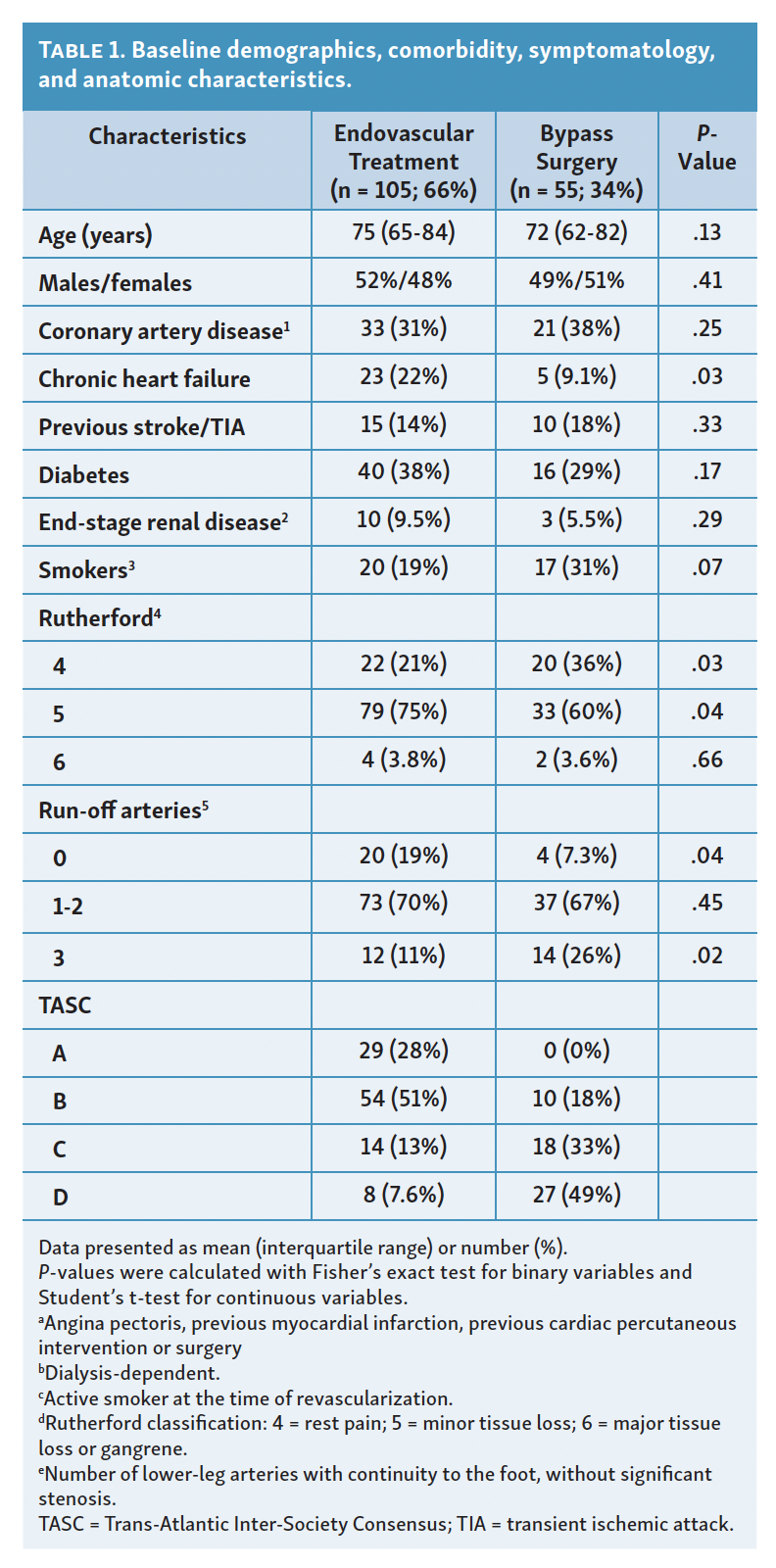
Patients and treatments. A flow chart of patients participating in the study is shown in Figure 1. Four patients were lost to follow-up, while the remaining 156 patients were followed for 2 years. Details regarding patient demographics, risk factors and comorbidities, as well as lesion characteristics and performed interventions are described in Table 1. Endovascular treatment was performed in 105 patients. Primary stenting was reserved for suboptimal angioplasty results and was performed in 22 cases. Bypass surgery was performed in 55 patients. Autologous vein was the preferred graft material and was used in 40 cases, whereas 12 patients had a synthetic graft and 3 had composite grafts due to inappropriate vein material. Patients who underwent bypass surgery had more complex femoropoliteal lesions (TASC C and D), in consistency with the TASC II revascularization recommendations, but the endovascular group had more extensive infrapopliteal atherosclerosis (Table 1). The common femoral artery was the most common site of proximal anastomosis (42 patients) and the popliteal artery was the most common site of distal anastomosis (16 patients above knee, 22 below knee, and 17 in the infrapopliteal arteries).
{kind=link}
{kind=link}


Clinical outcomes. Clinical outcomes at 2 years following the index revascularization have been previously reported.29 In summary, 22 patients in the endovascular group and 5 patients in the bypass group died (22% vs 11%, respectively; P=.08) and 19 patients in the endovascular group and 6 patients in the bypass group had a major lower-limb amputation (20% vs 11%, respectively; P=.13) over the 2-year follow up. Amputation-free survival at 2 years was 59% in the endovascular group vs 78% in the bypass group (P<.05). Among the patients subjected to amputation, the mean time from primary intervention to amputation was 83 days (95% CI, 43-124) in the endovascular group vs 310 days (95% CI, 97-524) in the bypass group (P<.05). The number of patients who underwent reintervention within 2 years was similar between treatment groups (41% vs 42%; P=.55), but the crude number of reinterventions per patient was higher in the bypass group (mean 0.88 vs 0.60 in the endovascular group; P=.09).
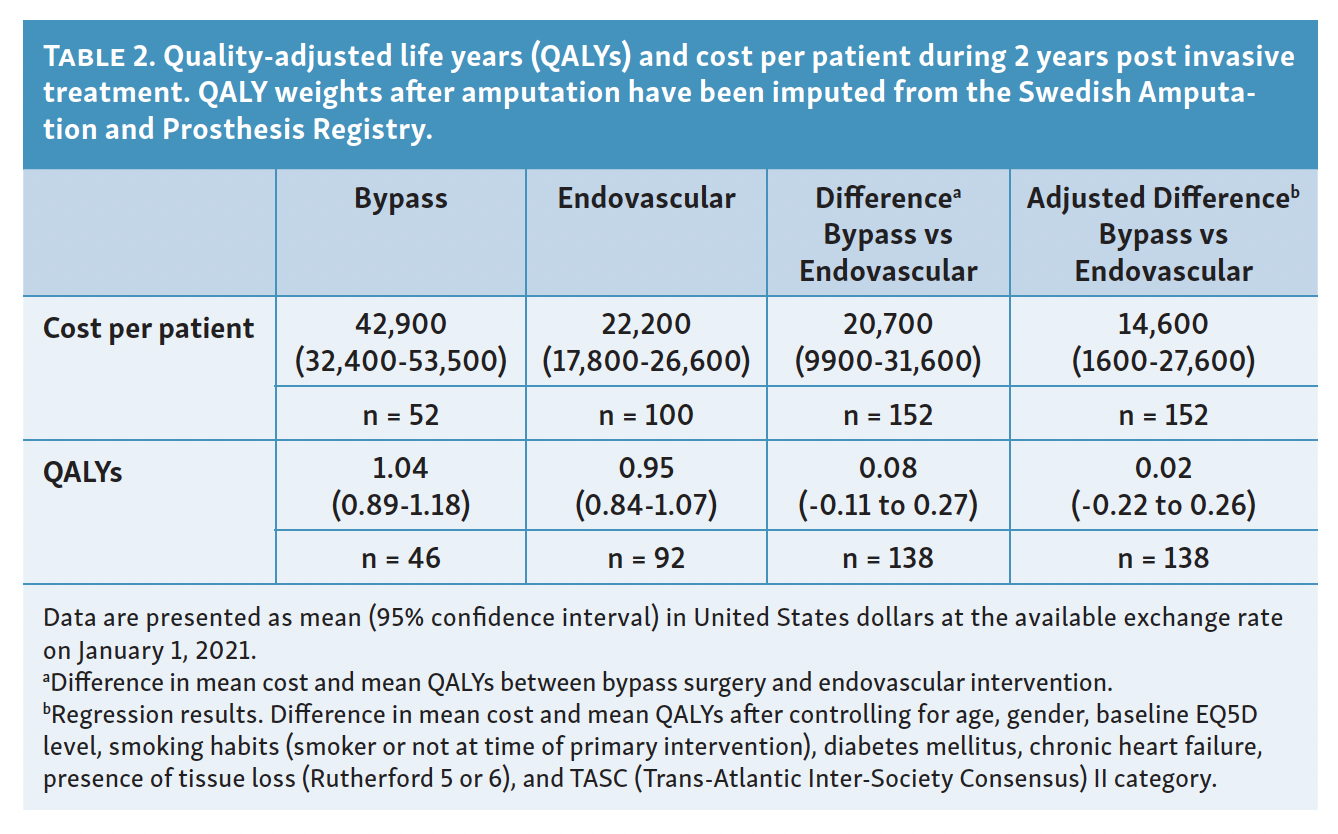
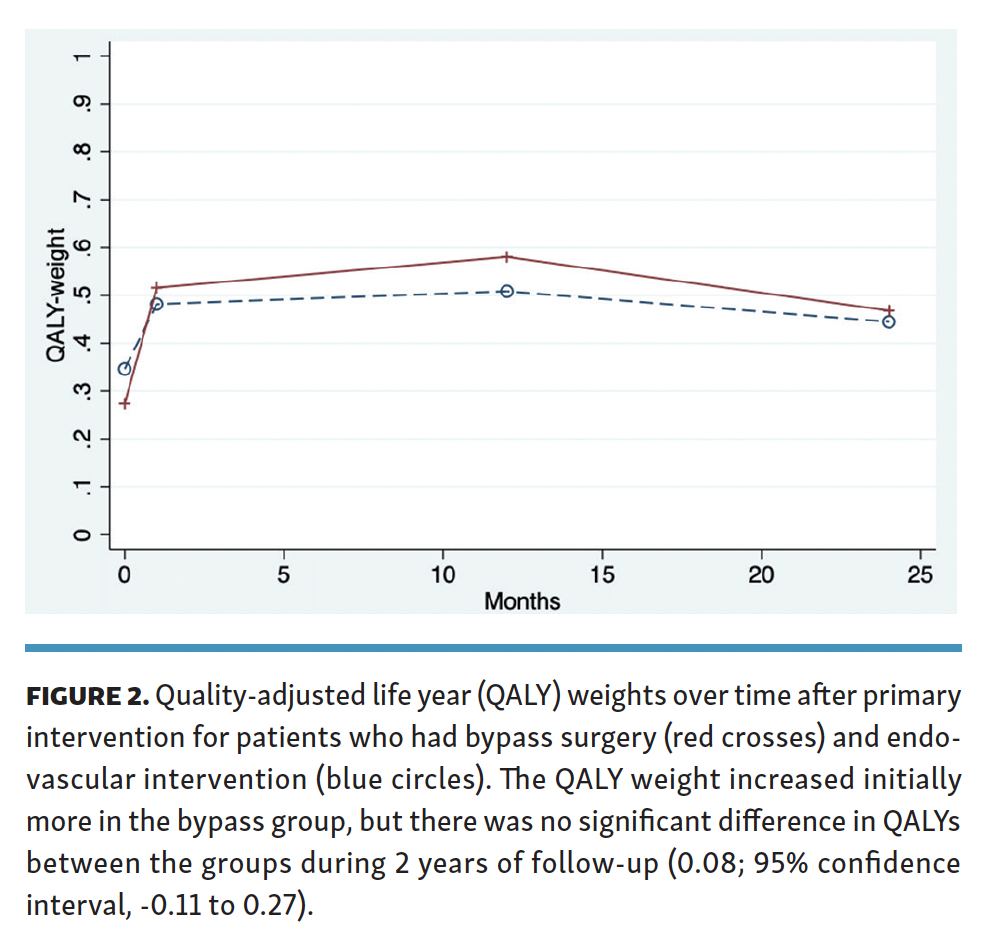
Quality of life. Health-status data were missing on 14 patients who did not completely fill out the EQ-5D questionnaire (6 in the bypass group and 8 in the endovascular group). The mean QALYs during the 2-year follow-up were 1.04 years (95% CI, 0.89-1.18) in the bypass group and 0.95 years (95% CI, 0.84-1.07) in the endovascular group (Table 2 and Figure 2). There was no significant difference in QALYs between treatment arms (bypass vs endovascular, 0.08; 95% CI, -0.11 to 0.27). A linear multiple regression model controlling for age, gender, baseline EQ-5D level, smoking habits, diabetes mellitus, chronic heart failure, presence of tissue loss (Rutherford 5 or 6), and TASC II category demonstrated a statistically nonsignificant difference in QALYs between the groups (bypass vs endovascular intervention, 0.02; 95% CI, -0.22 to 0.26). The only covariate in the regression model that affected mean QALYs during follow-up was the baseline EQ-5D index value (QALY weight).
{kind=link}
{kind=link}


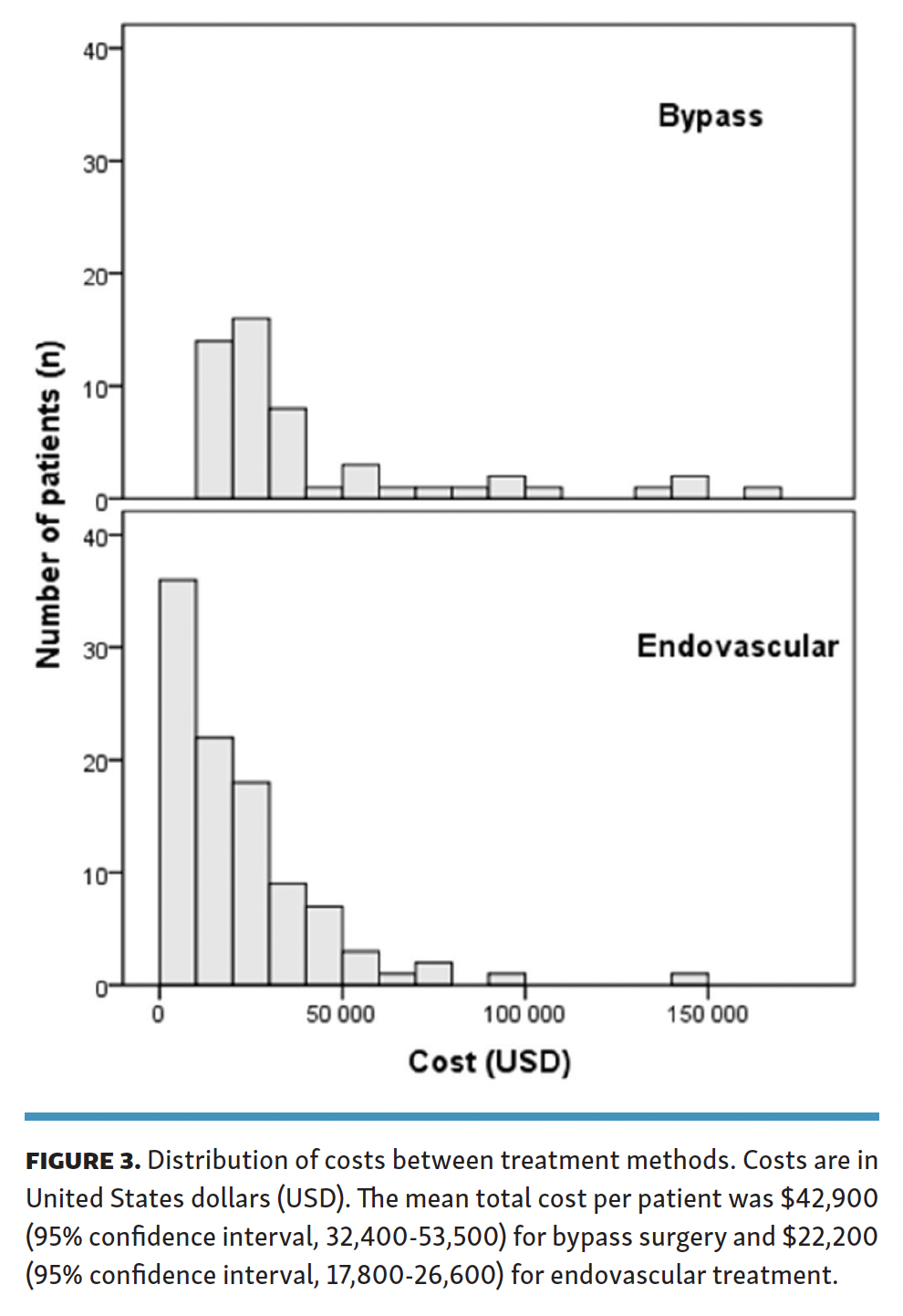
Treatment costs and ICER. The mean total cost per patient at 2 years was $42,900 (95% CI, 32,400-53,500) for bypass surgery and $22,200 (95% CI, 17,800-26,600) for endovascular treatment, resulting in a difference of $20,700 (95% CI, 9900-31,600) between the 2 treatment methods. Costs for hospital admissions and readmissions dominated ($40,500 in the bypass group vs $20,000 in the endovascular group) while costs for outpatient visits constituted a minor part of the total costs. As shown in Figure 3, the distribution of costs was skewed, with most observations in the lower range, as generally seen in cost data. Subgroup analysis on the patients subjected to major limb amputation during the study period showed substantially higher costs in the bypass group ($101,800; 95% CI, 41,300-162,200) vs the endovascular group ($42,600; 95% CI, 33,400-51,900). Excluding the subgroup of patients who died during the study period and thus did not generate further costs only marginally increased the mean total cost per patient ($44,700 for bypass surgery vs $24,400 for endovascular treatment). A linear multiple regression analysis on total costs, corresponding to the regression analysis performed on QALYs, resulted in a smaller cost difference between the 2 treatment groups ($14,600; 95% CI, 1600-27,600). Treatment method was the only covariate in the regression model that significantly affected costs per patient. The substantial cost difference between treatment methods, alongside a very small observed difference in QALYs, translated into a high ICER of $730,000 per QALY gained with bypass surgery. The difference in amputation rate between treatment methods, adjusted to the same set of covariates as described for QALYs and costs, translated to a cost per avoided major amputation with bypass surgery of $104,000.
{kind=link}

Discussion
In this prospective cohort study undertaken in CLTI patients with a principal target lesion in the femoropopliteal segment and who were treated with bypass surgery or endovascular intervention according to the TASC II recommendations, the cumulative hospital cost throughout 2 years of follow-up was almost twice as high for bypass surgery as for endovascular treatment. This is commensurate with reports from other cost analyses, although the literature is heterogeneous in terms of patient populations, cost data, and outcomes.16, 21-23 Hospitalization has previously been determined to be a main cost driver, which was also the case in this study, emphasizing the importance of reintervention rates.2,30 Although the percentage of patients subjected to reintervention within 2 years was similar after bypass surgery and endovascular intervention, the actual number of reinterventions per patient was higher in the bypass group, which likely contributed to the higher cumulative cost observed for bypass surgery. Patients subjected to amputation generated costs about twice as high as those for patients with preserved limbs. Although this relates to a limited number of patients, it is evident that amputation is also a main cost driver.
The main outcome measure in this cost-effectiveness analysis was generic health-related quality of life. Despite a general interest in patient-reported outcome measures in CLTI evaluations, cost-effectiveness analyses relating health-care costs to patient-reported quality of life are rare. In this study, patient-reported EQ-5D-3L questionnaires generated a numerically very small QALY difference between treatment methods, despite a substantial difference in overall amputation-free survival. The small difference in QALYs alongside the higher costs attributable to bypass surgery resulted in a very high ICER, well above all commonly accepted willingness-to-pay thresholds published,31,32 insinuating that bypass surgery targeting femoropopliteal lesions should not be considered a cost-effective treatment option for CLTI. However, despite being one of the most commonly used measures of health status in health economic evaluations, the ability of the EQ-5D-3L questionnaire to detect small changes in health status with enough sensitivity has been questioned. Since the start of this study, a 5 scale steps version of the questionnaire has been developed (EQ-5D-5L), but there is limited evidence for the use of this version in cost-effectiveness analyses.26 Presumably, disease-specific assessment tools such as the Vascular Quality of Life questionnaire (VascuQoL), the Peripheral Artery Questionnaire (PAQ), and the Peripheral Artery Disease Quality of Life (PADQOL) questionnaire would be more sensitive in reflecting health-status changes in this patient group, but to the best of our knowledge, there are no available tariffs to produce QALY weights from such PAD-specific questionnaires to be used in cost-effectiveness analyses.33-35
Despite the small difference in health-related quality of life between treatment groups in this study, we found a non-negligible difference in amputation-free survival. Both mortality and amputation rates were higher in the endovascular group, indicating that the endovascular group may have been burdened with more pronounced comorbidity. However, when adjusting for known and potential confounders as described in the methods section, amputation rates remained lower after bypass surgery. The numerically lower amputation rate with bypass surgery in relation to the higher costs resulted in an additional cost per avoided amputation with bypass surgery at approximately $104,000. Even if preventing amputation would generally be considered the main aim with CLTI interventions, this price tag is not easily interpreted. There are no specific willingness-to-pay thresholds with which to relate, and few previous publications on the topic. The closest comparison may be the Dutch cost-effectiveness analysis by Vossen et al, which reported an extra cost per 3 years of patency at €560,000 with bypass surgery compared with endovascular intervention in femoropoliteal lesions in a mixed population of claudication and CLTI.23 The technical development that has taken place mainly in the endovascular field since the start of our study may presumably have affected both patency and amputation rates as well as costs, rendering the net effect in terms of cost-effectiveness unclear and in need of further study.
To compensate for the non-randomized design of the present study, regression analyses were conducted both on costs and patient-reported health status. When adjusting for observed intergroup differences at baseline as well as the extent of the vessel lesions, as described in the methods section, the difference between treatment groups was less prominent both in terms of costs and health-related quality of life. Notably, the only variable in the cost-regression model that had any material impact on accumulated costs was the initial revascularization method. In the corresponding regression on health status data, only baseline QALY level had an impact on subsequent health status. In general, the QALY levels in this study demonstrate a low health status, comparable to many other chronic conditions and some cancer diagnoses.36 It may be assumed that some CLTI patients with overall poor health status will not benefit from the superior amputation-free survival rates demonstrated with bypass surgery. Yet, in patients with a reasonable baseline health status, better long-term results may motivate the additional initial costs with bypass surgery. This is in line with the conclusions from the BASIL trial, which recommended bypass surgery to patients with a life expectancy exceeding 2 years.37 Further studies are warranted to more precisely outline clinical algorithms that can select patients likely to benefit from bypass surgery, and where bypass surgery may still be a cost-effective treatment option.
Study strengths and limitations. The strengths of the current study include its prospective design and the use of prospectively collected actual per-patient costs. Also, evaluations were undertaken exclusively on CLTI patients. Many previous cost-effectiveness analyses have included both patients with intermittent claudication and CLTI, which may skew the results and in the end limit distinct conclusions as they are dependent on disease severity.19-23 Compared with patients with claudication, older age and more-pronounced comorbidity status in CLTI patients likely have a substantial impact on costs.
This study also has limitations. First, self-reported health-status data collection was ended after amputation, which needs to be recognized as an important limitation in terms of study design. For the purpose of analysis, previously reported health-related quality-of-life data from the Swedish Amputation and Prosthesis Registry were therefore imputed. In this registry, 85% of the patients are reportedly amputated due to diabetes or other vascular causes, and this may hence be considered an accurate data source that aligns well with our study population. Second, EQ-5D-3L questionnaires were incomplete in 14 cases (9%) that were consequently withdrawn from analysis. There is a risk that this data loss could be skewed toward the more frail patients with worse level of function and possibly worse quality of life. Third, a limitation in the collection of costs was that the hospital cost database does not allow for costs to be separated between departments during a single hospital stay and thus, as described, necessitated cost approximations in a limited number of cases. Nor does the dataset allow for costs to be separated into procedural, material, and staff costs. Fourth, the nonrandomized design introduces a risk of residual confounding, but multivariable regression analysis demonstrated that our main results were overall robust when controlling for known or potential confounders. Finally, it should be emphasized that cost analyses in this study refer to in- and outpatient hospital costs and that primary health-care costs, other societal and patient costs, as well as costs accrued beyond the study period of 2 years were not considered.
Conclusion
Among patients with CLTI and the main target lesion in the femoropopliteal segment, treated invasively according to the TASC II recommendations, those who underwent bypass surgery generated almost 2 times the total hospital costs as patients who underwent endovascular intervention throughout 2 years of follow-up. A higher reintervention rate in the bypass group is likely to be a contributor to the higher costs associated with bypass surgery. Amputation-free survival was favorable among patients who underwent bypass surgery in this nonrandomized study, but a corresponding generic health-status gain could not be demonstrated when using the EQ-5D-3L questionnaire. This translated to a substantial additional cost per gained QALY and per avoided amputation with bypass surgery compared with endovascular intervention.
Affiliations and Disclosures
From the 1Department of Vascular Surgery, Sahlgrenska University Hospital and Institute of Medicine, Department of Molecular and Clinical Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; and 2School of Public Health and Community Medicine, Institute of Medicine, University of Gothenburg, Gothenburg, Sweden.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Nordanstig reports payment for lectures from Bayer, BD, and Medtronic; travel support from BD; advisory board for Bayer (all unrelated to the current study). The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted January 27, 2022.
Address for correspondence: Angelica Perlander, MD, Department of Vascular Surgery, Sahlgrenska University Hospital, Bruna Stråket 11b, SE-413 45 Gothenburg, Sweden. Email: angelica.perlander@vgregion.se