A First Case of Successful Intervention of Axillary Artery Chronic Total Occlusion Using the Pantheris Device
Ibrahim Halil Inanc, MD1; Vasili Lendel, MD2; Kostas Marmagkiolis, MD3; Cezar Iliescu, MD3; Ismail Ates, MD4; Thomas E. Milner, PhD5; Nitesh Katta, PhD, MSc, BTech, MTech5; Marc David Feldman, MD6; Mehmet Cilingiroglu, MD3
ISSN: 2694-3026
J CRIT LIMB ISCHEM 2022;2(3):E64-E66. Epub 2022 August 29. doi: 10.25270/jcli/CLIG22-00010
Abstract
Background. Peripheral arterial disease (PAD) is a clinical manifestation of systemic atherosclerosis and is associated with significant morbidity and mortality. Despite the novel treatment modalities for endovascular revascularization, the optimal treatment strategy remains challenging. Intravascular optical coherence tomography (IV-OCT) is an imaging modality that offers a detailed visualization of the blood vessel wall microstructure. The Pantheris device (Avinger), an integrated version of IV-OCT in a directional atherectomy device, has been used for the revascularization of lower extremity occlusions. We present a 73-year-old patient with chronic total occlusion of the axillary artery with successful revascularization using the Pantheris device, for the first time in the literature.
J CRIT LIMB ISCHEM 2022;2(3):E64-E66. Epub 2022 August 29. doi: 10.25270/jcli/CLIG22-00010
Key words: chronic total occlusion, intravascular optical coherence tomography, new devices
Introduction
Peripheral arterial disease (PAD) represents the second-most common manifestation of atherosclerosis, with a prevalence of 5.6% in 2015, affecting more than 230 million people worldwide; it is associated with a significantly increased risk of coronary artery disease (CAD) and stroke.1 PAD mostly involves the lower-extremity vessels, but can also involve the upper-extremity, mesenteric, and renal arteries. Depending on the degree of chronic narrowing of each vascular area, a range of symptoms such as intermittent claudication may occur or, in acute thrombosis cases, may lead to critical limb ischemia.2,3
Despite the optimal use of novel technologies, such as orbital or rotational atherectomy, new-generation stents, drug-eluting stents, drug-coated balloons, and covered stents for endovascular revascularization, restenosis remains at long-term follow-up.4 Intravascular optical coherence tomography (IV-OCT) is an optical analog of intravascular ultrasound (IVUS), using near-infrared light instead of sound to obtain cross-sectional images of the artery, and enabling the visualization of blood vessel wall microstructure in vivo with an unprecedented level of detail.5 Although it is more commonly used in CAD interventions, IV-OCT can also provide important information for predicting future events after the procedure, as well as informing the procedures utilized in PAD interventions.5-9 Herein, we present a patient with chronic total occlusion (CTO) of the axillary artery who underwent revascularization using the Pantheris rotational atherectomy device (Avinger), for the first time in the literature.
Case Description

A 73-year-old female patient was admitted due to left upper-limb claudication during minimal work and dyspnea during exercise (class II), but angina was not present. Her complaints were present for 1 year but had increased in the last 2 months. She was a smoker and had a history of diabetes mellitus, hypertension, and dyslipidemia. During the physical examination, left brachial and radial pulses were not palpable. Blood pressure was recorded as 140/85 mm Hg from the right arm, but could not be recorded from the left arm. Both arms were warm, without any discoloration or gangrenous changes. Doppler ultrasound imaging revealed an occlusion of the left axillary artery and damped, monophasic, delayed time to peak, broad systolic peak, and continuous diastolic flow waveform below the occlusion site. Coronary angiography showed atherosclerotic changes of the coronary arteries without any significant occlusive disease.

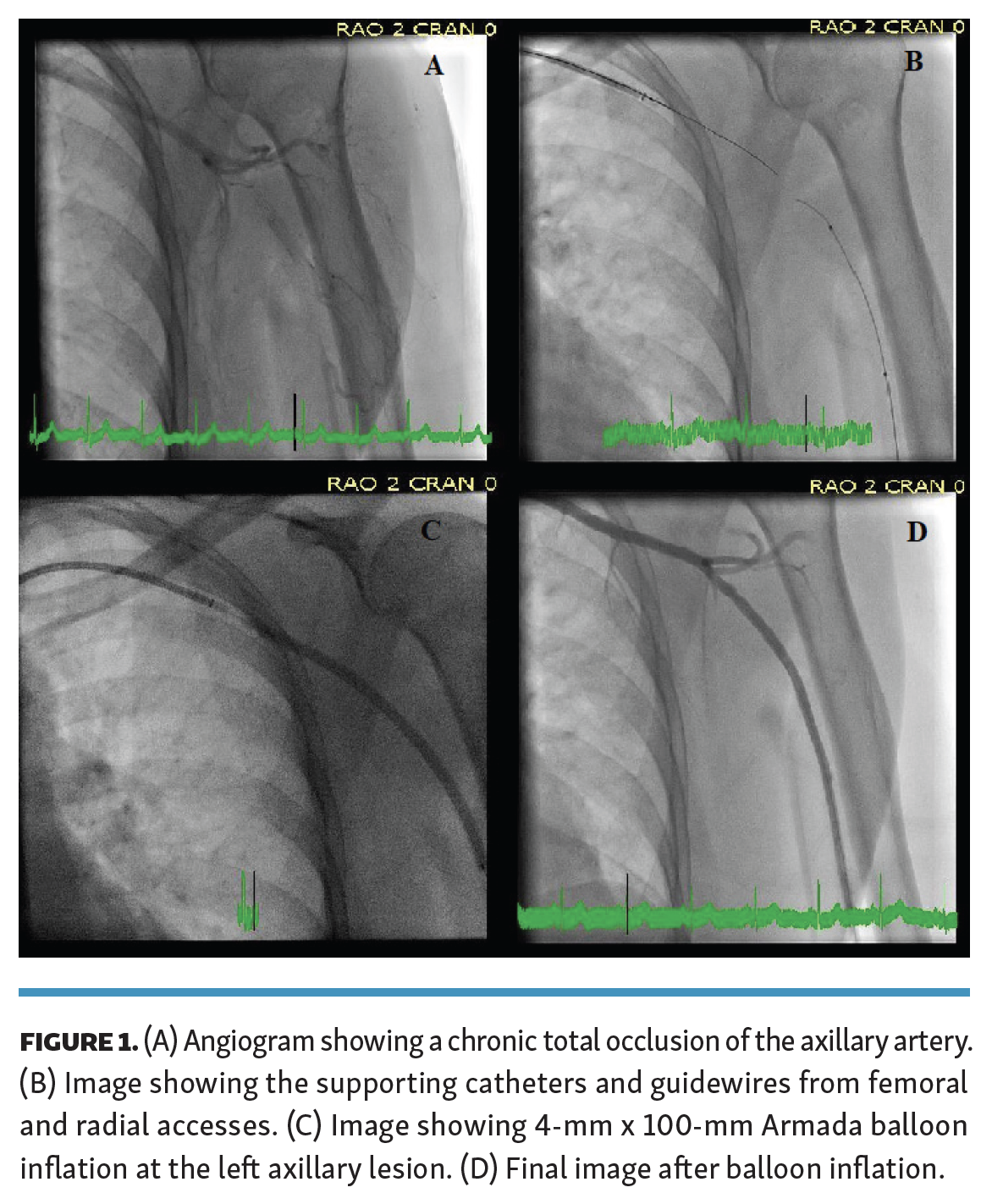
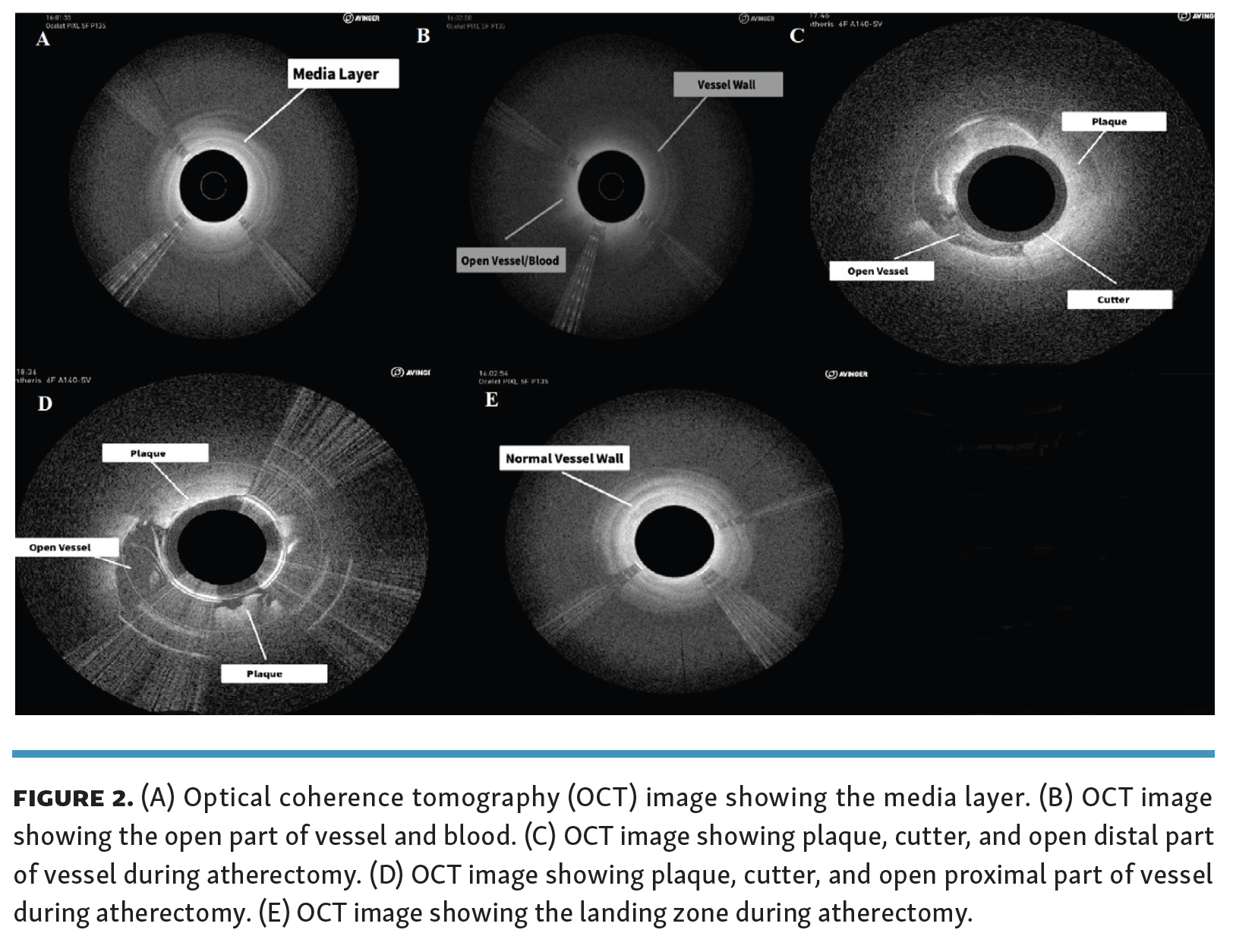
Left upper-extremity images showed the CTO of the axillary artery and an endovascular intervention was planned for the occlusion (Figure 1A). A 6-Fr, 6-cm x 90-cm sheath and 6-Fr slender sheath were used for femoral and left radial artery accesses, respectively. During the procedure, 4-Fr Seeker support catheter (Philips) and Sion black, Mongo, and Astato guidewires (all Asahi Intecc) were used via femoral access. Five-Fr Viance (Medtronic), Quick-cross (Philips), and Ocelot support catheters (Avinger) and Sion black, Astato, and Glidewire guidewires (Terumo)were used via radial access (Figure 1B). A 300-cm Regalia guidewire (Asahi Intecc) was used for externalization via femoral access. The Pantheris SV was advanced over the Regalia guidewire to the left axillary artery via femoral access for the atherectomy and OCT images (Figures 2A-2E). A 4-mm x 100-mm Armada balloon (Abbott Cardiovascular) was inflated at the left axillary and axillary/proximal brachial lesions at 10 atm for 180 seconds and at the left at 6 atm for 180 seconds after atherectomy, respectively (Figure 1C). The intervention was completed without any complications (Figure 1D). Left brachial and radial artery pulses were palpable after the procedure. During 4-week follow-up at the clinic, patient had complete relief of her symptoms.
{kind=link}
{kind=link}
Discussion
Currently, endovascular intervention has been increasingly used for the treatment of PAD. However, in addition to acute technical success, long-term vessel patency after the intervention remains key.8,10 Recurrent symptoms, clinical events, and repeated procedures may be encountered following PAD interventions due to restenosis. Therefore, it is important to understand the underlying vascular pathology, identify complications such as vessel dissection and plaque protrusion, and to prevent restenosis.11
Both IVUS and IV-OCT help to understand the lesion characteristics, measure the true diameter of the vessel, guide the selection of the optimal stent length, define the landing site more precisely, identify complications, and provide important clues regarding the physiopathology of acute and late restenosis in patients undergoing intervention for CAD. In this way, they provide better clinical outcomes in the long term.12 OCT seems to be disadvantageous compared with IVUS in large vessels due to the need for blood clearing. Further, more limited soft tissue penetration in the presence of red thrombi, lipid, or necrotic core that reduces light penetration is another limitation of IV-OCT compared with IVUS. On the other hand, IV-OCT has 10-times higher axial resolution and provides a more detailed imaging of the histopathological structure of the underlying plaque.12
Recently, the Pantheris device, an integrated version of IV-OCT in a directional atherectomy device, has been used for the revascularization of lower-extremity occlusions.13,14 Axial and longitudinal views provide detailed information on plaque characterization and load. An important advantage is that the system allows the removal of plaque while reducing vessel injury without damaging the normal wall of the vessel, especially the adventitial layer.10 The VISION (Evaluation of the Pantheris Atherectomy System) trial,13 which was a multicenter, single-arm study that included 158 patients, the safety and efficacy of revascularization under the guidance of a Pantheris atherectomy catheter with integrated IV-OCT system was investigated in the treatment of patients with symptomatic femoropopliteal disease. The primary safety endpoint was the composite of major adverse events within 6 months. Tissue samples from each intervened lesion were histologically analyzed to evaluate the accuracy and precision of the OCT image guide. Major adverse events occured in 16.6% of patients, with a very low procedural complication rate. Importantly, plaque burden in OCT-guided lesions was significantly greater than the expected plaque burden evaluated by fluoroscopy. In another study, Memon et al14 investigated the procedural and clinical outcomes of Pantheris device-guided intervention for femoropopliteal CTO lesions in patients with chronic kidney disease. They found that Pantheris device-guided interventions were associated with less use of contrast agents, total fluoroscopy time, and radiation exposure.
Conclusion
Pantheris device-guided peripheral artery intervention offers a detailed evaluation of the underlying vascular pathology, such as dissection, neointimal proliferation, neoatherosclerosis, and degree of calcification, reduces the complication risk of the interventional procedure by minimizing adventitial injury, and guides the optimal clinical and procedural outcomes in real time. Its use for the revascularization of upper-extremity occlusions as well as lower-extremity occlusions may provide significant benefits. Further randomized clinical studies are needed.
Disclosures
From 1Kırıkkale Yuksek Ihtisas Hospital, Department of Cardiology, Kırıkkale, Turkey; 1Arkansas Heart Hospital, Department of Cardiology, Little Rock, Arkansas; 3University of Texas in Houston, MD Anderson Cancer Center, Houston, Texas; 4Department of Cardiology, Sisli Konan International Hospital, Istanbul, Turkey; 5Beckman Laser Institute and Medical Clinic, University of California-Irvine, Irvine, California; and the 6Department of Cardiology, UT Health San Antonio, San Antonio, Texas.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted August 18, 2022.
Address for correspondence: Mehmet Cilingiroglu, MD, FSCAI, FACC, FAHA, FESC, UT Houston, MD Anderson Cancer Center, Houston, TX, University of Arkansas, School of Biomedical Engineering, Fayetteville, AR 72701. Email: Cilingiroglumehmet@gmail.com