Limb Salvage Endovascular Technique in Chronic Limb-Threatening Ischemia
Ahmad Hallak, MD; Ayman Nasir, MD; William Bennett, MD, PhD; Zola N’Dandu, MD
ISSN: 2694-3026
J CRIT LIMB ISCHEM 2022;2(3):E67-E73. Epub 2022 September 20. doi: 10.25270/jcli/CLIG22-00003
Abstract
Peripheral artery disease (PAD) remains a significant contributor to morbidity and mortality in the United States. Chronic limb-threatening ischemia is the late stage of PAD and is associated with high rates of amputation. Advancements in surgical and endovascular therapies have been successful in reperfusion and limb salvage. This case report describes a successful endovascular revascularization technique which, along with a multidisciplinary approach, resulted in limb salvage with only a minor amputation.
J CRIT LIMB ISCHEM 2022;2(3):E67-E73. Epub 2022 September 20. doi: 10.25270/jcli/CLIG22-00003
Key words: critical limb ischemia, limb salvage
Introduction
Peripheral artery disease (PAD) remains a significant contributor to morbidity and mortality in the United States. Chronic limb-threatening ischemia (CLTI) is the late stage of PAD and is associated with high amputation rates. Advancements in surgical and endovascular therapies have been successful in reperfusion and limb salvage. This case report describes a successful endovascular revascularization technique which, along with a multidisciplinary approach, resulted in limb salvage with only a minor amputation in order to demonstrate the feasibility of revascularizing a patient with CLTI with extensive multilevel disease and showcases the technical aspects of the procedure.
Case Description
A 63-year-old female with PAD (Fontaine III, Rutherford 4), coronary artery disease, hypertension, hyperlipidemia, stroke without residual neurologic deficits, and a 60-pack year smoking history presented with progressively worsening right foot severe rest pain for a week. She had a pertinent history of peripheral vascular intervention for acute right-limb ischemia treated with catheter-directed thrombolysis and subsequent stenting of the superficial femoral artery (SFA) with two 6- x 60-mm Smart stents (Cordis), 4- x 60-mm Xpert stent (Abbott) extending from the distal P3 popliteal artery (POP) into the proximal anterior tibial artery (ATA), and a 3- x 40-mm Xpert stent in the mid ATA 9 years prior to the index presentation. At this admission, she had a left transfemoral distal aortogram with selective right-leg angiography, which revealed 75% stenosis in the right common iliac artery (CIA) and in-stent chronic total occlusion (CTO) of the right SFA extending through the entire popliteal artery with severe infrapopliteal disease. She had a single-vessel runoff on the right with a chronically occluded ATA filling from geniculate collaterals without good visualization of inframalleolar vessels due to motion artifact because of severe pain. The tibioperoneal trunk (TPT), proximal peroneal artery (PRA), and entire posterior tibial artery (PTA) were chronically occluded with a faintly filling lateral plantar artery. Initially, an endovascular approach was chosen for revascularization. The right SFA in-stent CTO was not crossed with antegrade 4-Fr Glide catheter (Terumo) and .035˝ Glide wire (Cordis) manipulation.
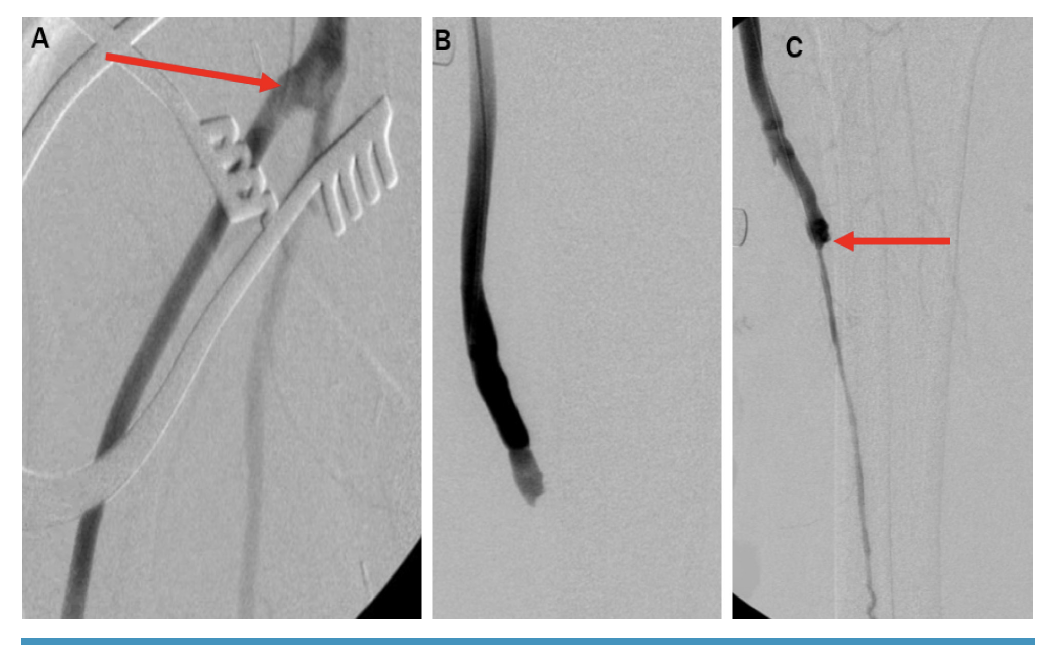
After discussion of the treatment options and with a goal of limb salvage, she was evaluated for bypass surgery even though the outflow target vessel was not ideal as the distal bed was not well visualized. She underwent right common femoral artery (CFA) to ATA bypass with a nonreversed saphenous vein harvested from the left leg (Figure 1). Arterial Doppler the next day revealed occlusion of the bypass due to poor outflow. Without a residual autologous conduit, she was no longer an ideal surgical candidate and was discharged with follow-up in the wound care clinic. Her tissue oximetry was 3 mm Hg on the dorsum and 23 mm Hg on the medial aspect of the foot, below the healing threshold.
{kind=link}

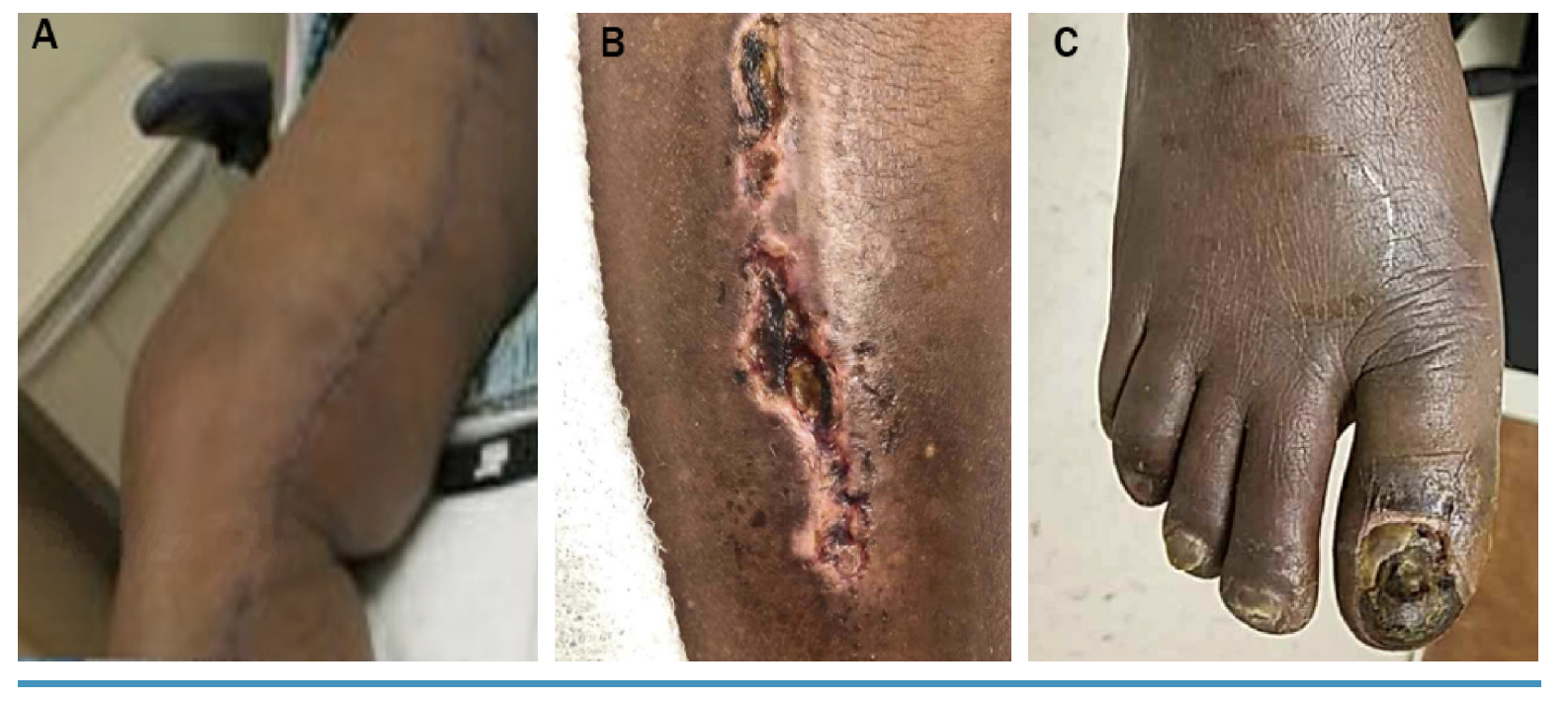
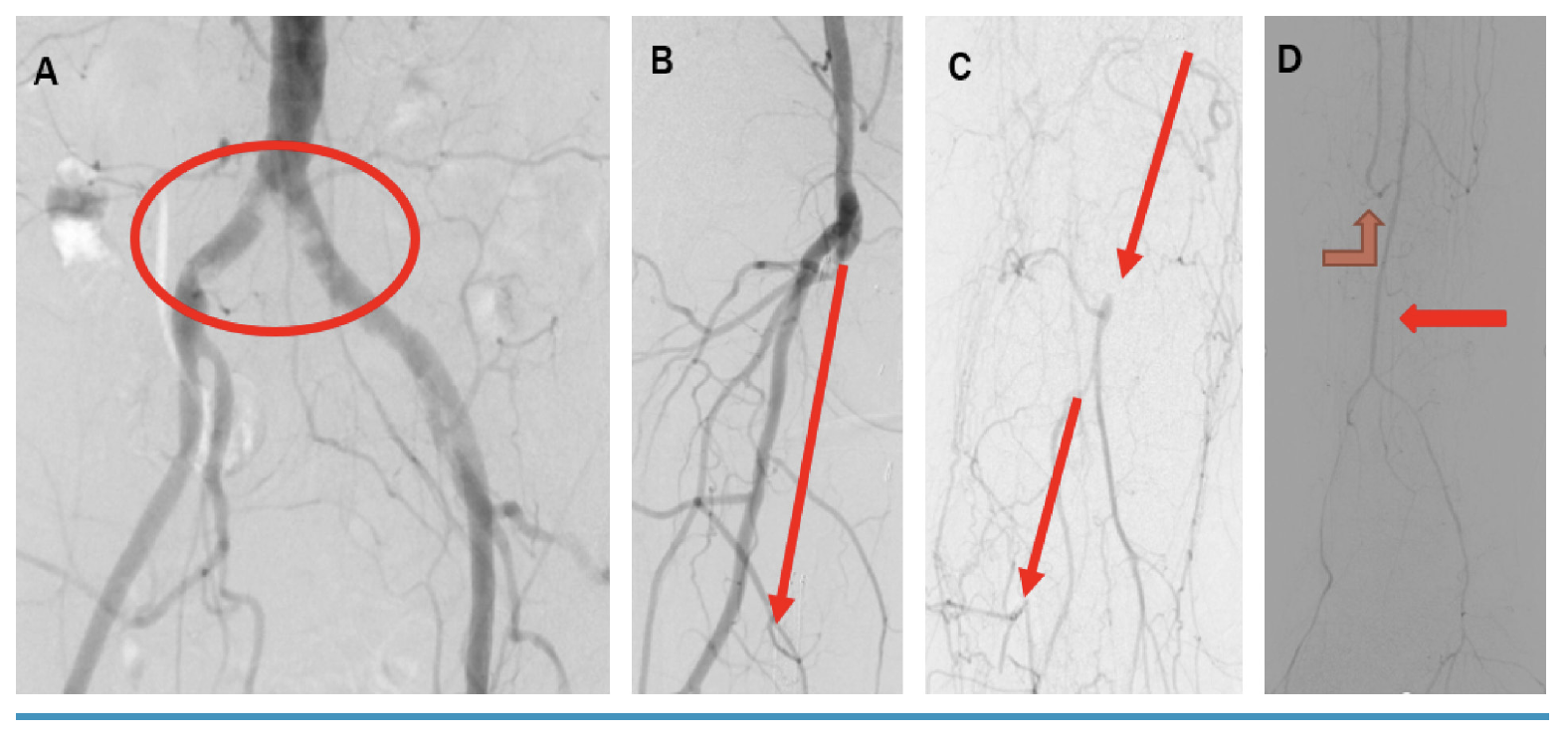
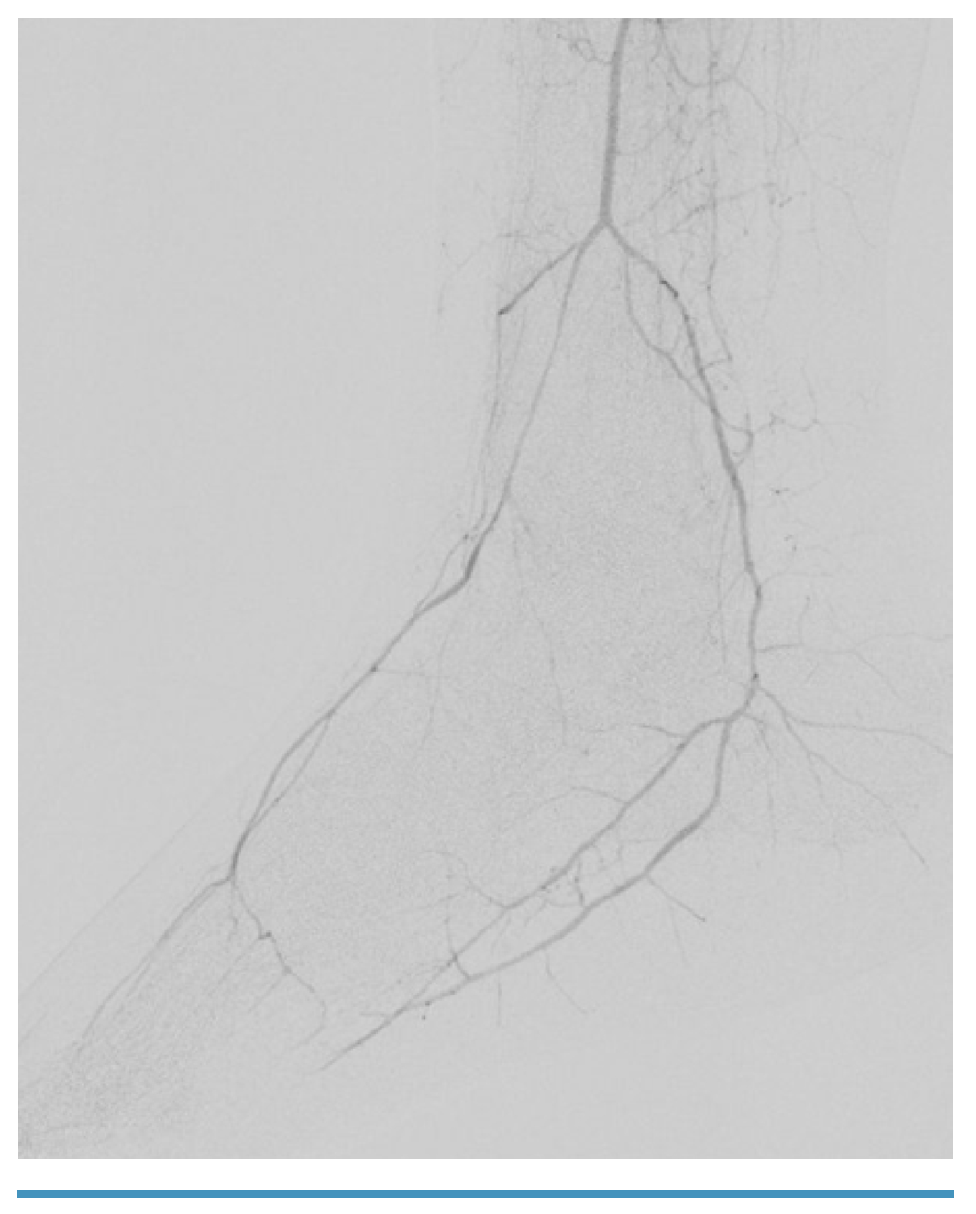
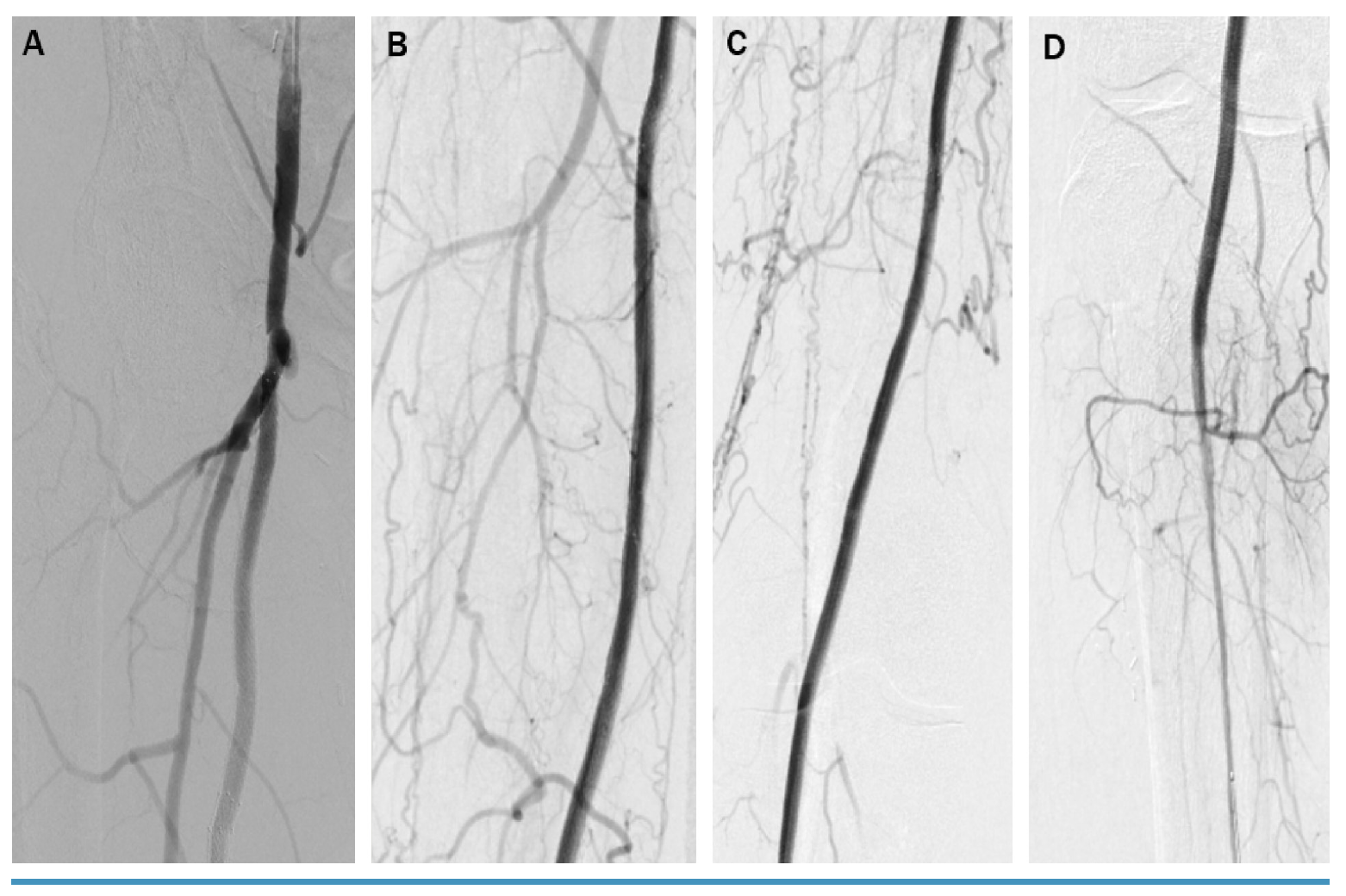
One month after her admission, she developed a right great toe ulcer with early ischemic changes in the 4th toe, which was now Fontaine IV, Rutherford 5 (Figure 2). Her care team referred her to our center for revascularization. In an attempt to salvage her limb, she underwent another angiogram with general anesthesia to eliminate any motion artifact due to pain. The study revealed 75% right common iliac artery (CIA) disease, proximal SFA in-stent CTO with a concave proximal cap, P1 to P3 segment POP-CTO, mid right ATA in-stent CTO, PTA-CTO, and TPT-CTO with distal reconstitution of PRA from an anterior communicator branch of the ATA. PRA provided collaterals to the distal PTA and dorsalis pedis artery (DPA), forming an intact palmar arch (Figure 3 and Figure 4).
{kind=link}
{kind=link}
{kind=link}



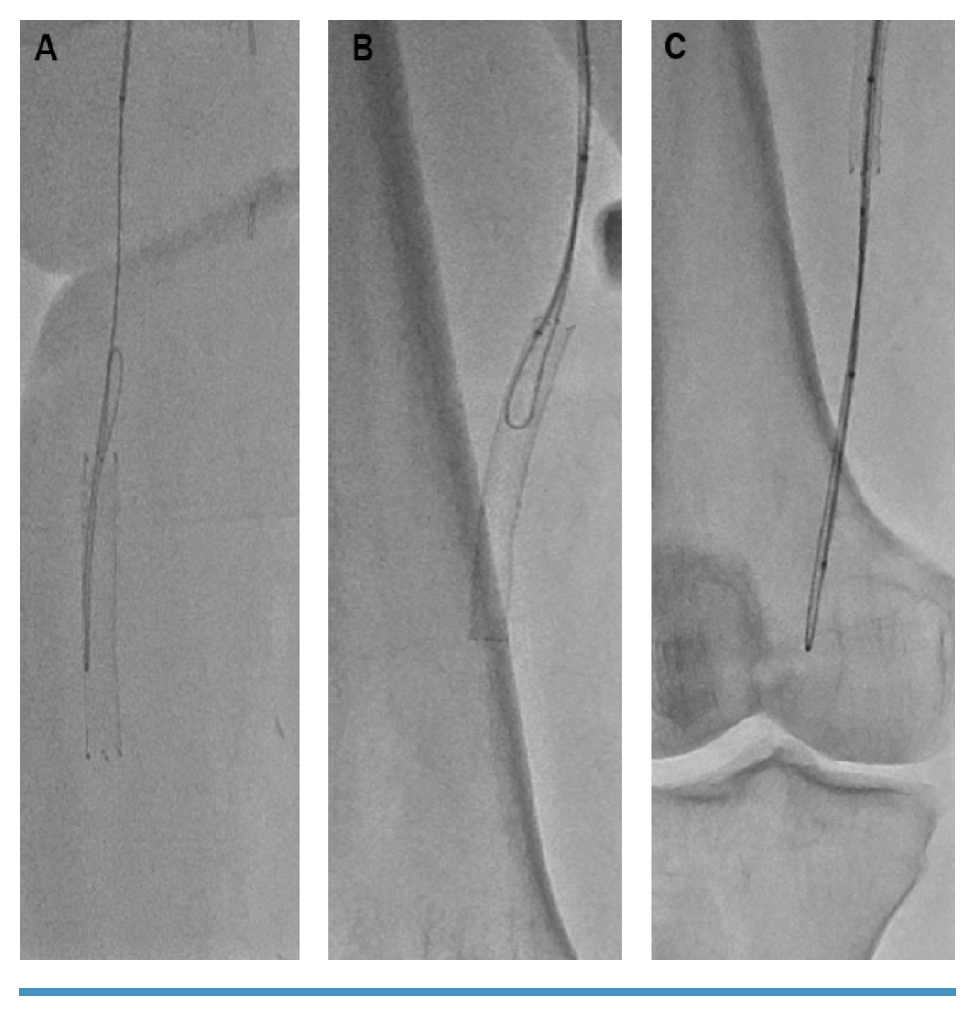
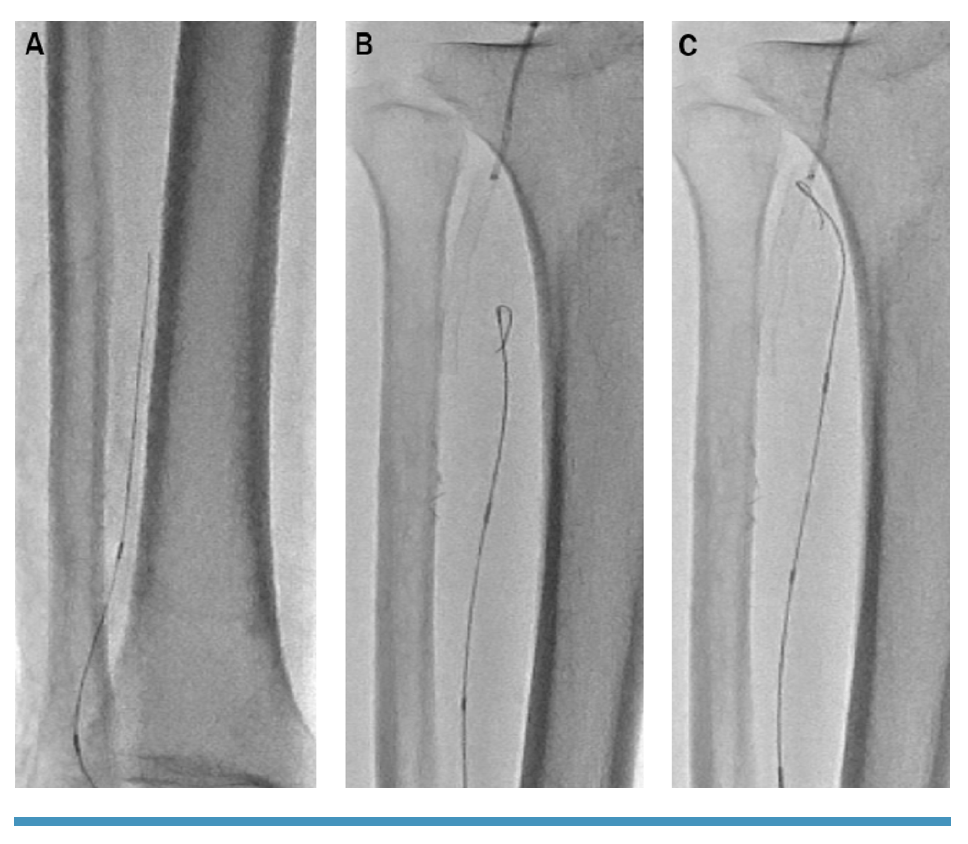
She was re-evaluated for revascularization to prevent a major amputation. The new strategy was based on antegrade and retrograde access with possible subintimal flossing with delivery of therapy from the antegrade access. The retrograde access was obtained to assist with crossing of the extensive multilevel disease. Extravascular ultrasound (EVUS)-guided left CFA and retrograde right DPA were obtained. A 7-Fr x 45-cm Destination sheath (Terumo) was inserted in the left CFA and a retrograde 2.9-Fr micropuncture pedal sheath (Cook Medical) was inserted in the right DPA. The combination of an angulated, 150-cm, .035˝ Navicross (Terumo) with 0.035” Glidewire Advantage support catheter (Terumo) crossed the proximal SFA-CTO cap intraluminally then crossed subintimally from the mid SFA to the P3 POP artery segment. Through the retrograde 2.9-Fr micropuncture pedal sheath, an .018˝ CXI support catheter (Cook Medical) and an .014˝ Fielder XT wire (Asahi Intecc) were advanced through the DPA into the anterior malleolar collateral into the PRA for rendezvous with the antegrade catheter in the ostial TPT for wire externalization. After removal of the Fielder XT wire, a V18 wire (Boston Scientific) was inserted through the retrograde .018˝ CXI support catheter and advanced in the antegrade .035˝ Navicross catheter (Figure 5 and Figure 6). We established subintimal arterial flossing with antegrade-retrograde intervention (SAFARI technique) in the TPT through the struts of the previously deployed stent extending from the distal POP to the proximal ATA with a 330-cm-long, .014˝ ViperWire. An .014˝ Eagle Eye intravascular ultrasound (IVUS) catheter (Philips) was inserted for additional evaluation and to determine the optimal treatment. IVUS revealed moderate circumferential plaque, subintimal SFA and POP crossing, and intraluminal PRA crossing with re-entry in the TPT. An Emboshield NAV6 distal embolic filter (Abbott) was placed in the distal PRA to protect the single vessel to the foot. The PRA was predilated with a 3.5- x 150-mm Ultraverse balloon (BD). The TPT was predilated with a 4.0- x 150-mm Ultraverse balloon. The POP was serially predilated with 4.0- x 150-mm, 5.0- x 150-mm, and 6.0- x 150-mm Ultraverse balloons. The SFA was serially predilated with 5.0- x 150-mm, 6- x 150-mm, and 7- x 150-mm Ultraverse balloons.
{kind=link}
{kind=link}


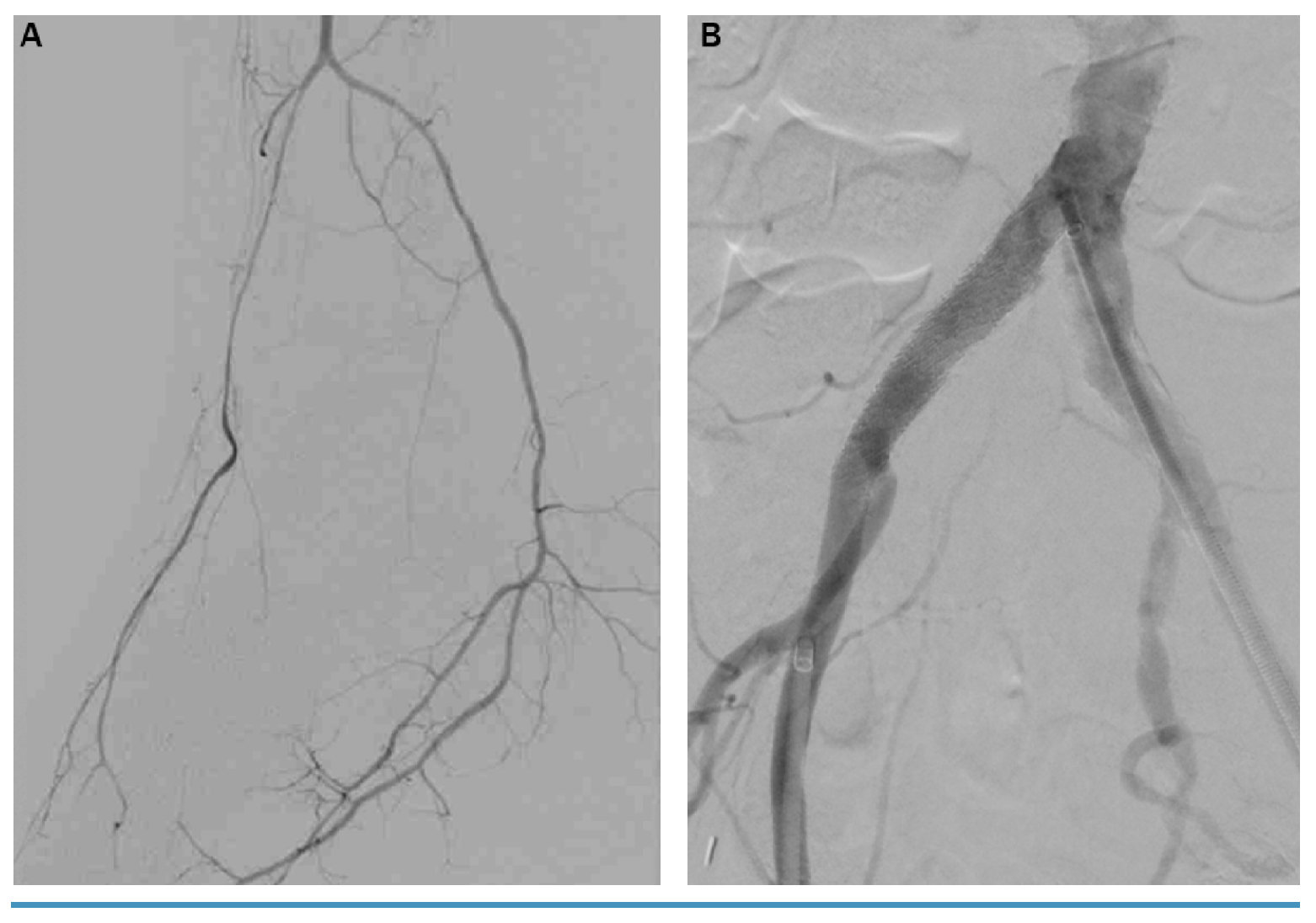
Ultimately, stents were deployed from the proximal PRA to the proximal SFA, starting with a 3.5- x 38-mm Resolute (Medtronic) drug-eluting stent, a 4.0- x 38-mm Resolute drug-eluting stent postdilated with a 5.0-mm balloon, a 5.5- x 150-mm Supera stent (Abbott), a 6.0- x 150-mm Supera stent, and a 7- x 140-mm Zilver PTX stent (Cook Medical). Finally, the right CIA was treated with an 8- x 56-mm Valeo balloon-expandable stent (BD Bard) postdilated with a 10-mm balloon (Figure 7 and Figure 8). IVUS revealed well-apposed stents. After removal of the filter, hemostasis of the left CFA was achieved with a ProGlide closure device (Abbott) and manual pressure for the retrograde DPA access.
{kind=link}
{kind=link}


The patient was discharged on aspirin, clopidogrel, atorvastatin, and losartan. She was referred to a smoking cessation program and wound care. She underwent partial right great toe amputation, which healed after 3 months of aggressive wound care (Figure 9).
{kind=link}

Discussion
CLTI has an incidence of 0.35% and prevalence of 1.33%.1 Several factors influence the choice of revascularization modality, including patient characteristics, lesion characteristics, local expertise, referral patterns, and operator preference. The input of a multidisciplinary team, including surgeons and endovascular specialists among other specialties, ensures that all revascularization options are considered and all contributing factors of CLTI are addressed. While the multidisciplinary team approach has not been studied in a randomized trial, limited observational data suggest improved outcomes and lower amputation rates.2-4
There are several technical features unique to our case. Our ability to obtain ultrasound-guided access of a faintly filling or hibernating DPA. Surgical interventions can be challenging in CLTI patients because of long-segment and multivessel occlusions, lack of adequate targets, dense calcification, and few pedal outflow channels. As a result, innovative endovascular techniques like retrograde arterial canalization via reconstituted pedal vessels should be considered for successful revascularization. Using the CTO crossing approach based on plaque morphology (CTOP classification), our patient’s CTO was type II which describes a proximal concave cap and a distal convex cap.5 The utility of the CTOP classification was beneficial in planning our intervention for a successful procedural outcome. This route may allow lesion traversal where it would otherwise not be possible, laying the path for primary retrograde revascularization or rendezvous techniques and subsequent antegrade intervention.1
The SAFARI technique is also an important highlight. Combined retrograde and antegrade interventions trace back to the “Bolia” technique,7 initially described for femoropopliteal interventions in which the recanalized channel was intraluminal or subintimal. There was eventual crossing of a retrograde wire into an antegrade catheter, allowing wire rendezvous and antegrade intervention. These techniques have more recently been deemed helpful in CLTI patients with CTOs that cannot be crossed with antegrade or subintimal re-entry techniques.8
The Supera stent was chosen for its high flexibility, high kink resistance, and high torsional strength to address the various dynamic changes that occur in the distal superficial femoral and popliteal artery, such as shortening, twisting, bending, and compression (Figure 10). Additionally its innovative, interwoven-nitinol and mimetic design generate a high radial strength needed in this particular case to maintain an open lumen across the crushed struts of the previously deployed Xpert stent extending from the P3 popliteal to the proximal ATA jailing the ostium of the TPT.9
{kind=link}

Conclusion
Revascularization is the cornerstone of the treatment of CLTI. There are multiple options, eg, surgical interventions, endovascular interventions, or a combination of both procedures. The complexity of CLTI requires a multidisciplinary team approach to deliver comprehensive care. A multidisciplinary team approach fosters a patient-centered culture and ensures that every pathological factor contributing to this complex disease process is addressed and followed by the corresponding specialist, leading to the most successful possible outcome for patients, physicians, and healthcare systems.10 This case demonstrates the ability to revascularize a patient with CLTI with extensive multilevel disease and showcases the technical aspects of the procedure.
References
1. Nehler MR, Duval S, Diao, L, et al. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J Vasc Surg. 2014;60(3):686-695.e2. doi:10.1016/j.jvs.2014.03.290
2. Chung J, Modrall JG, Ahn C, Lavery LA, Valentine RJ. Multidisciplinary care improves amputation-free survival in patients with chronic critical limb ischemia. J Vasc Surg. 2015;61(1):162-169. Epub 2014 Jul 26. doi:10.1016/j.jvs.2014.05.101
3. Hioki H, Miyashita Y, Miura T, et al. Prognostic improvement by multidisciplinary therapy in patients with critical limb ischemia. Angiology. 2015;66(2):187-194. Epub 2014 Feb 26. doi:10.1177/0003319714523113
4. Kolte D, Parikh S, Piazza G, et al. Vascular teams in peripheral vascular disease. J Am Coll Cardiol. 2019;73(19):2477-2486. doi:10.1016/j.jacc.2019.03.463
5. Saab F, Jaff MR, Diaz-Sandoval L, et al. Chronic total occlusion crossing approach based on plaque cap morphology: the CTOP classification. J Endovasc Ther. 2018;25(3):284-291. Epub 2018 Feb 27. doi:10.1177/1526602818759333
6. Vraux H, Hammer F, Verhelst R, Goffette P, Vandeleene B. Subintimal angioplasty of tibial vessel occlusions in the treatment of critical limb ischemia: mid-term results. Eur J Vasc Endovasc Surg. 2000;20(5):441-446. doi:10.1053/ejvs.2000.1200
7. Bolia A, Sayer RD, Thompson MM, Bell PR. Subintimal and intraluminal recanalization of occluded crural arteries by percutaneous balloon angioplasty. Eur J Vasc Surg. 1994;8(2):214-219. doi:10.1016/s0950-821x(05)80463-3
8. Manzi M, Palena LM. Retrograde percutaneous transmetatarsal artery access: new approach for extreme revascularization in challenging cases of critical limb ischemia. Cardiovasc Intervent Radiol. 2013;36(2):554-557 Epub 2012 Apr 25. doi:10.1007/s00270-012-0391-3
9. Hioki H, Miyashita Y, Miura T, et al. Prognostic improvement by multidisciplinary therapy in patients with critical limb ischemia. Angiology. 2015;66(2):187-194. Epub 2014 Feb 26. doi:10.1177/0003319714523113
10. Shishehbor MH, White CJ, Gray BH, et al. Critical limb ischemia: an expert statement. J Am Coll Cardiol. 2016;68(18):2002-2015. Epub 2016 Sep 28. doi:10.1016/j.jacc.2016.04.071
Disclosures
From Ochsner Medical System, New Orleans, Louisiana.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted September 13, 2022.
Address for correspondence: Ahmad Hallak, MD, Ochsner Medical System, 1514 Jeff Hwy, New Orleans, LA 70121. Email: aohallak@outlook.com