A Novel Temporary Stent For Treatment of Infrapopliteal Arteries in Conjunction With Drug-Coated Balloon Angioplasty: The DEEPER Pilot Study
Jihad A. Mustapha, MD1; Ammar Ibrahim, MD2; Fadi Saab, MD3; Jos van den Berg, MD, PhD4; Andrew Holden, MBChB, FRANCZCR, EBIR5; Carolyn Mascho, BSN, DNP, RN, AG-NP6
ISSN: 2694-3026
J CRIT LIMB ISCHEM 2022;2(3):E83-E91. Epub 2022 August 15. doi: 10.25270/jcli/CLIG22-00007
Abstract
Abstract
Background. Treatment of peripheral arterial disease (PAD) of the infrapopliteal arteries with endovascular therapy is hampered by high restenosis rates. This temporary stent is a novel device developed to address the challenges of infrapopliteal disease. Objectives. The objectives of this trial were to evaluate the safety and performance of the temporary stent in treating infrapopliteal arterial disease. Methods. The trial was a prospective, single-center, nonrandomized feasibility study, with angiographic and ultrasound core-laboratory adjudication. In total, 23 subjects with infrapopliteal artery disease, Rutherford class 3-5, were treated with the investigational device. Analysis was conducted by the per-protocol (PP) group and the intent-to-treat (ITT) group. Eighteen lesions in 17 subjects were included in the PP analysis. Subjects were followed at 1-, 3-, 6-, and 12-month follow-up visits. Results. The primary efficacy endpoint results demonstrated 88.9% patency by Duplex ultrasound in the temporary stent + drug-coated balloon PP cohort (n = 17 subjects, 18 lesions). One subject underwent target-lesion revascularization (5.6%; n = 18) and 0 subjects (0%; n = 17) underwent major amputation. There were no deaths during the trial and no major adverse limb events (major amputation) occurred in the first 30 days in any patients. Conclusion. The temporary stent shows promise as a safe and effective method for the treatment of infrapopliteal arterial disease, with exceptional patency results and a comparable safety profile. Further research should be conducted to establish efficacy and confirm safety.
J CRIT LIMB ISCHEM 2022;2(3):E83-E91. Epub 2022 August 15. doi: 10.25270/jcli/CLIG22-00007
Key words: amputation, infrapopliteal arterial disease, infrapopliteal stenting, peripheral arterial disease
Introduction
Current treatment options for peripheral arterial disease (PAD) and critical limb ischemia (CLI) consist of surgical or endovascular revascularization of occluded or stenosed infrapopliteal arteries. The anatomy of the tibial vessels renders both surgical and endovascular treatments complex. Surgical bypass requires adequate target vessels for distal anastomosis, and patients may not be candidates because of lack of available vein conduit or other comorbidities.1 Endovascular interventions are increasingly used for these patients, with percutaneous transluminal balloon angioplasty (PTA) being the most common treatment approach. PTA is associated with more rapid restenosis rates than bypass, although limb salvage is comparable.2-4
Endovascular treatment of infrapopliteal arteries was initially performed with coronary devices, and to this day coronary stents are used off-label in the infrapopliteal arteries due to a lack of infrapopliteal-specific stents. However, the arterial anatomy and nature of atherosclerotic disease are significantly different in the infrapopliteal arteries than in the coronary arteries. In addition to long lesion lengths and a more muscular arterial wall, infrapopliteal arteries have been found to have a higher rate of concentric and medial calcification (Mönckberg’s calcification) than coronary arteries.5
Drug-coated balloons (DCBs) have recently been explored as a treatment for infrapopliteal arteries, but penetration of drug into the intima and media is limited by the presence of concentric, medial calcification.6-8 A study by Fanelli et al found that any degree of calcium may affect the performance of DCBs and that circumferential calcification significantly impacts primary patency, with 50% of these lesions demonstrating restenosis at 12 months.6 Similar results were seen in the THUNDER trial; the strongest predictor of negative outcome was neither length nor location, but bilateral calcium.9 This suggests that treatment of calcified lesions with DCB only allows drug uptake into the noncalcified arterial wall segments. A second factor that contributes to restenosis is early vessel recoil, as was observed in 97% of subjects with CLI in a study by Baumann et al.10 Recoil and calcification are more prevalent in older patients with hypertension, diabetes, and chronic kidney disease, who comprise the vast majority of CLI patients.7,10
The use of drug-eluting stents has shown promise in treating infrapopliteal disease, with reported patency rates as high as 80% at 1 year.11 However, these trials have been conducted in short lesions, in the proximal arterial segments. Stent use in the infrapopliteal arteries remains limited by tibial anatomy, especially lesion length.10
The Temporary Spur Stent System (Reflow Medical) was developed specifically for the treatment of infrapopliteal disease. The purpose of this device is to provide a temporary mechanical scaffold that allows for controlled vessel expansion, with the intent to reduce vessel recoil and prevent significant dissection, with the benefits of a stent while leaving nothing behind in the body. The radial structures covering the stent penetrate the vessel wall, allowing for greater drug uptake into the vessel when followed by DCB (see Methods for detailed description). A single-center, nonrandomized feasibility study was designed in order to evaluate the safety and performance of the temporary stent, in conjunction with a commercially available DCB for the treatment of infrapopliteal PAD and CLI.
Methods
Study design. The DEEPER (A non-randomizeD fEasibility trial of the tEmporary stent for the treatment of lesions in the infraPoplitEal aRtery) trial was a nonrandomized, prospective, single-center feasibility study conducted under the CONABIOS (Consejo Nacional de Bioetica en Salud) institutional review board, the competent authority in the Dominican Republic. The study was carried out in accordance with the Declaration of Helsinki and good clinical practices. The investigational device was a temporary stent. Investigators treated target lesion(s) by predilation with plain balloon angioplasty, followed by the temporary stent and DCB. Independent angiographic (Syntropic) and ultrasound (Vascore) core labs were used for adjudication of angiographic and Duplex ultrasound imaging.
Study population. The clinical investigation was initiated on October 17, 2017, with the last patient follow-up performed on June 4, 2019. Qualifying subjects who gave informed consent were enrolled in a consecutive fashion. The study was open to subjects with PAD, Rutherford class 3-5, who were not pregnant, who were >18 years old, and who had a life expectancy of >1 year. They were recruited from a diabetic clinic located in the Dominican Republic. Primary inclusion criteria included Rutherford category 3-5, vessel diameter between 2.5 and 4.0 mm, target vessel located below the tibial plateau, with reconstitution above the level of the ankle, and total treated length ≤34 cm. Rutherford class 3 patients were permitted based on precedence of ongoing clinical trials of infrapopliteal disease.14

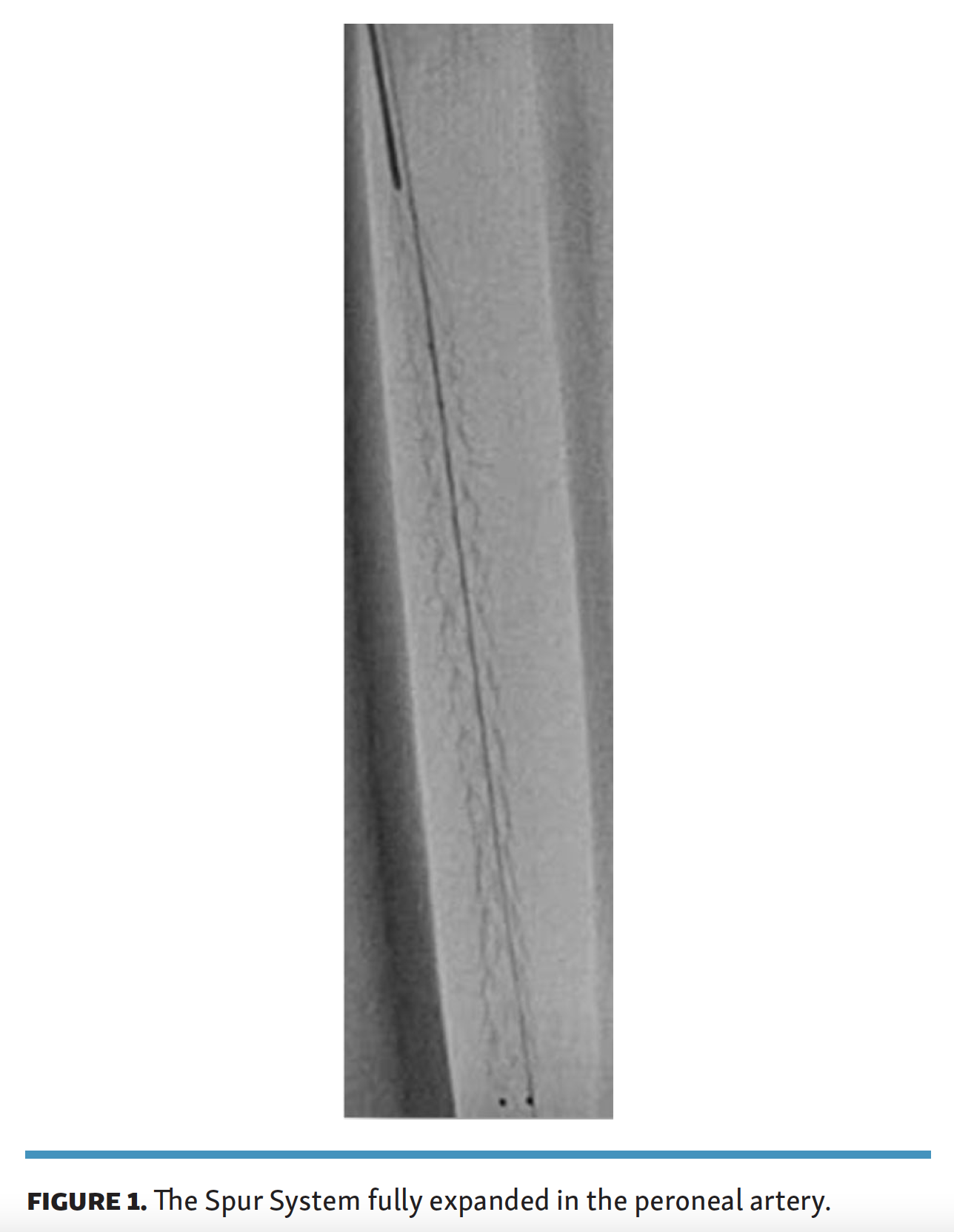
Study device. The temporary stent is an over-the-wire catheter with a 135-cm working length, compatible with 0.014˝ guidewires. The temporary stent consists of 2 catheters, the delivery catheter containing the temporary stent, and a retrieval catheter. The device is a nitinol, self-expanding stent, and is uniformly covered in radial structures that allow for penetration into the arterial wall (Figure 1). The stent is available in a length of 60 mm and 2 diameters, 3.0 mm (for 2.5-mm to 3.5-mm vessel diameters) and 4.0 mm (for 3.5-mm to 4.0-mm vessel diameters). The temporary stent is similar in design to other nitinol stents on the market in stent structure and delivery, but differs in that it is intended to be retrieved from the body, and not remain as a permanent implant following treatment.
{kind=link}

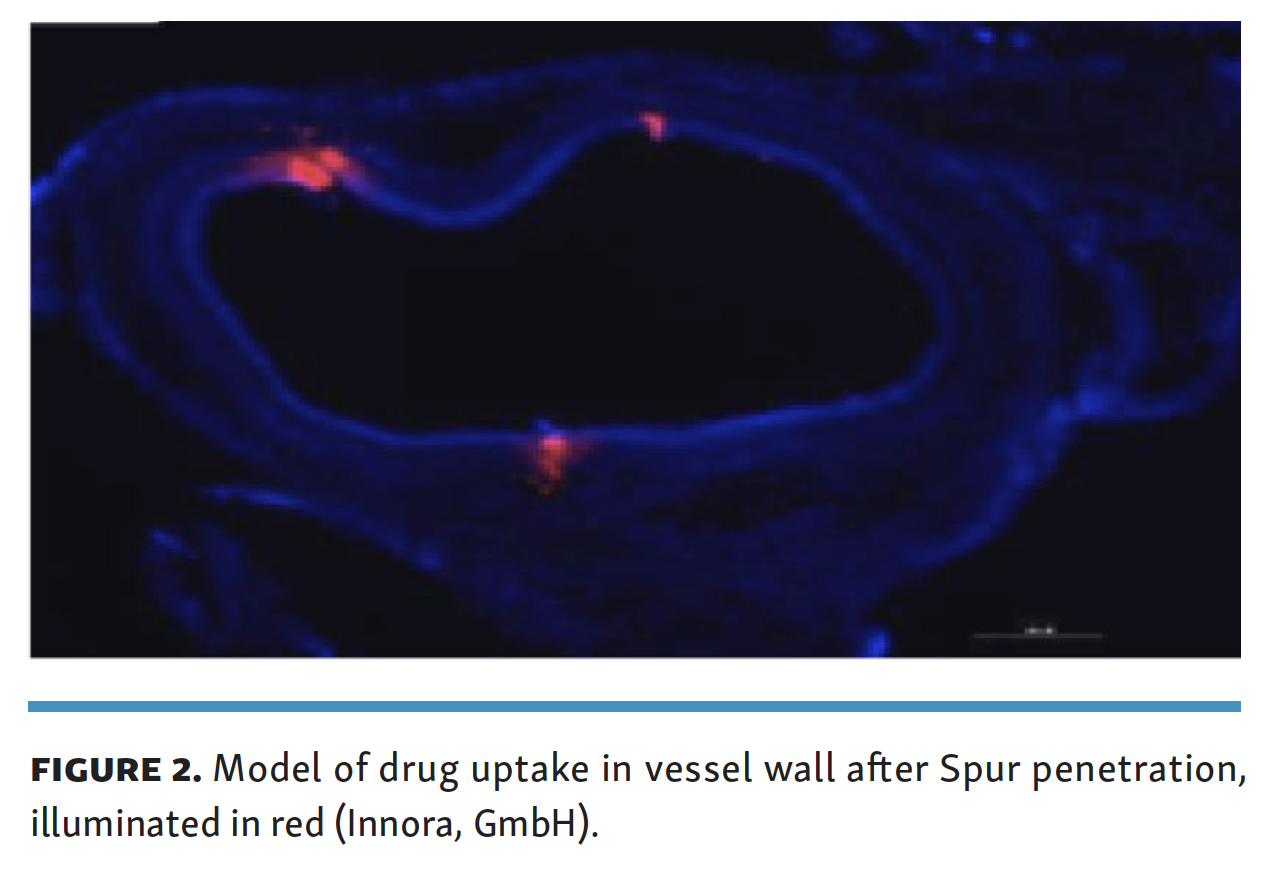
After deployment, the temporary stent is further dilated with a balloon, creating small channels in the vessel wall. These channels may alter the vessel wall to allow for greater uptake of antiproliferative drug, into the media, delivered via DCB (Figure 2). Stent scaffolding adds temporary structural support during balloon expansion, which is intended to reduce vessel recoil. The combination of these effects is intended to address 2 primary barriers to vessel patency in the infrapopliteal artery, ie, the immediate effect of vessel recoil and the longer-term effects of poor penetration of antiproliferative drug.
{kind=link}

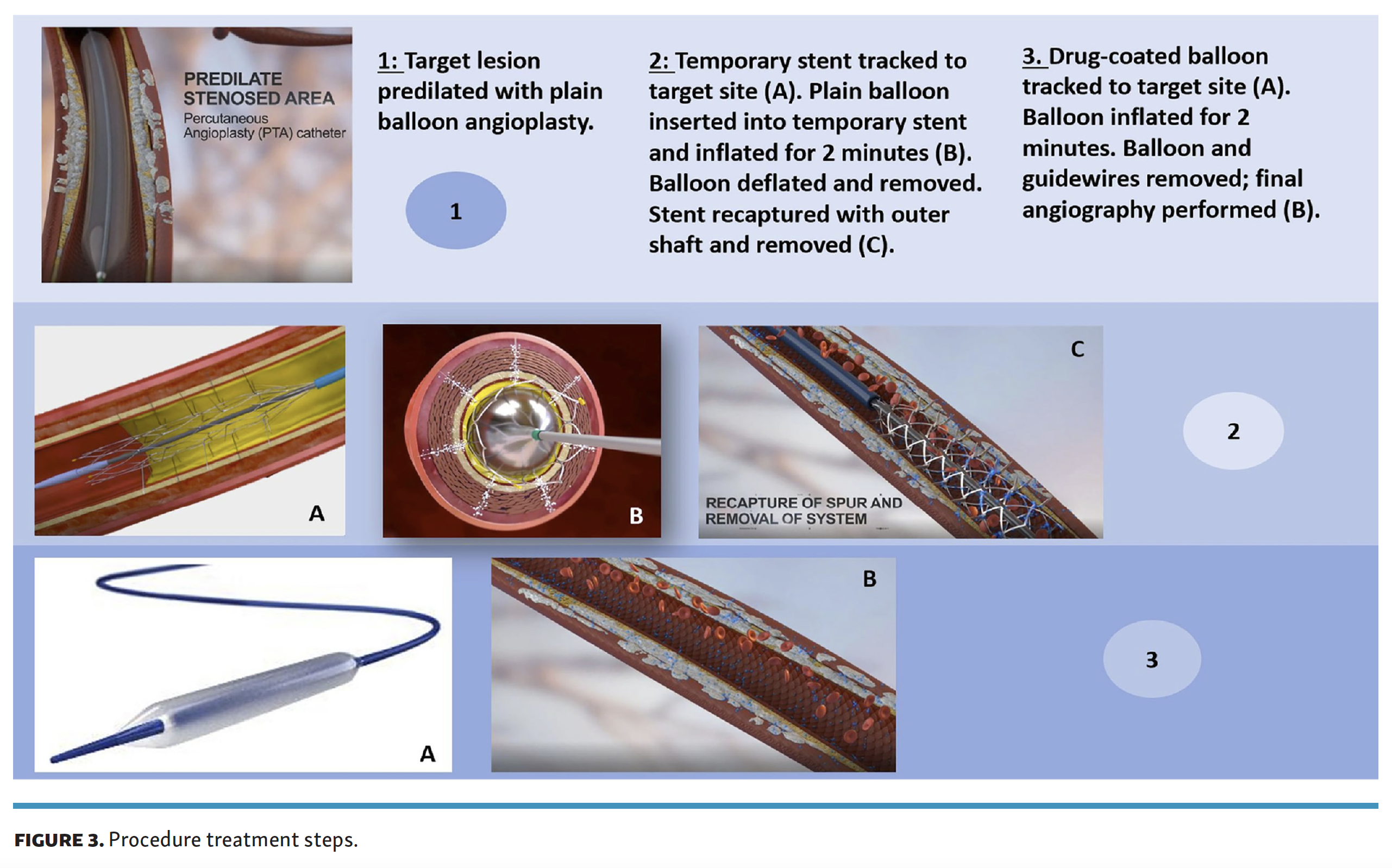
Study procedure. The procedure steps are outlined in Figure 3. An ipsilateral antegrade access was obtained and a 6-Fr sheath was inserted in the common femoral artery. Retrograde access was permitted for crossing, but the investigational device was deployed from antegrade access. Angiography was performed and the infrapopliteal lesion was identified. A radiopaque ruler was used in all images to avoid geographic miss. If present, inflow lesions were treated with plain balloon angioplasty.
{kind=link}
The target lesion was then crossed with a guidewire. Vessel diameter was visually estimated, and 1:1 predilation was performed with balloon angioplasty. Following successful predilation, defined as stenosis of <50%, and absence of thrombus, aneurysm, or flow-limiting dissection, the temporary stent was advanced over the .014˝ guidewire to the lesion site. Using a pin-pull method, the temporary stent was deployed at the target location. A plain balloon was then advanced through the temporary stent and inflated to nominal pressure for at least 2 minutes. The balloon was then deflated and removed. Subsequently, the retrieval catheter was advanced over the .014˝ guidewire, capturing the temporary stent, which was then removed from the vessel. Each temporary stent is single use. If the lesion length required the use of multiple temporary stents, overlapping treatments were utilized to avoid geographic miss.
Following treatment with the temporary stent, a commercially available DCB, the Lutonix .014 BTK (BD Bard), was deployed to the lesion site and inflated for at least 2 minutes. The segment that had been treated with the temporary stent was completely covered by the DCB in order to allow for penetration of the drug into the arterial wall channels created by the temporary stent. Dissections incurred during predilation were treated by performing standard prolonged inflation with the temporary stent, followed by prolonged DCB inflation up to 3 minutes. Bail-out stenting was permitted; however, no subjects required the use of a bail-out stent. Groin access was closed with a closure device under ultrasound. Subjects were started on dual-antiplatelet therapy (DAPT) with clopidogrel 75 mg once daily and aspirin 81 mg daily for 6 months.
Study follow-up. Within 24 hours after the procedure, subjects underwent ankle-brachial index (ABI) and toe-brachial index (TBI) testing, adverse event assessment, and Duplex ultrasound (DUS) evaluation. Subsequently, subjects returned to the study clinic for follow-up visits at 1 month, 3 months, 6 months, and 12 months. At these times, subjects underwent a physical exam, adverse event assessment, medication review, ABI and TBI testing (if applicable/available), as well as DUS testing. Twenty-two subjects underwent angiographic follow-up at 6 months.
Objectives and endpoints. The data analysis consisted of the intent-to treat (ITT) group, defined as all subjects who were treated with the temporary stent + DCB, regardless of protocol deviations, and the per-protocol (PP) group, consisting of subjects who did not have any angiographic protocol deviations. Angiographic protocol deviations included lesion length >34 cm and target vessels that did not reconstitute at or above the level of the ankle.
The primary effectiveness endpoint was to estimate the rate of target-lesion patency by continuous wave Doppler through 6 months. Patency was defined as the presence or absence of arterial flow through the entire length of the treated segment, based on the absolute peak systolic velocity (PSV) and/or PSV ratio data, in addition to the associated correlating factors supporting patency; presence of flow by color Doppler, and absence of post-stenotic waveform turbulence. This definition was selected because estimations of percent stenosis by PSV ratio alone in the infrapopliteal arteries are not well defined in the literature, and expert recommendations have been made for the evaluation of presence or absence of total occlusion in the infrapopliteal arteries, especially for subjects with CLI.12
The dual primary safety endpoints were freedom from device- and procedure-related death through 30 days post procedure, and freedom from target-limb major amputation and clinically driven target-lesion revascularization (CD-TLR) through 12 months post procedure. Secondary safety endpoints were freedom from major adverse limb events (MALEs; defined as amputation above the level of the ankle in the target limb) and all-cause perioperative death (POD) at 30 days.
Other outcomes analyzed included angiographic patency, defined as the presence or absence of flow through the treated segment, change in Rutherford class score, ABI and TBI, and wound healing. Demographics were analyzed for differences in race/ethnicity, sex, age, and comorbidities.
Vessel lumen diameter was analyzed by DUS at 24 hours, 1 month, 3 months, 6 months, and 12 months. This measurement was only considered to be accurate for subjects who maintained vessel patency. Studies included in this analysis had vessel diameter taken from a single measurement at the same location of the vessel at each visit. The percent change in lumen diameter was then calculated over time.
Statistical analysis. The PP group was identified as the primary analysis group, as there were no major protocol deviations in the group that may have affected outcomes. The effectiveness endpoint was analyzed by dividing the number of patent lesion sites by the number of treated lesions in the PP and ITT populations, respectively.
The safety endpoint of freedom from device- and procedure-related death through 30 days post procedure was analyzed by dividing the number of subjects who died by the total number of subjects in the PP and ITT populations, respectively.
The safety endpoint of freedom from MALE and CD-TLR through 12 months post procedure was analyzed by estimating the rate of major adverse events (CD-TLR and major amputation) through 1 year post procedure using a Kaplan-Meier analysis, in the PP and ITT populations. Continuous variables are expressed as mean (range) or median ± standard deviation; categorical variables are given as counts. Kaplan-Meier estimates were performed with Stata, version 1.4 (StataCorp) and descriptive statistics were performed with Excel, version 2002 (Microsoft).
Results









Patient follow-up and characteristics. All subjects returned for in-person follow-up visits through 6 months. Two subjects did not present in person for the 1-year visit, but were contacted by telephone. One of these subjects was reported as alive and in good health, without amputation or TLR, and the second subject reported major amputation of the index limb. Twenty-two subjects (23 lesions) were treated with temporary stent + DCB (the ITT population). Seventeen subjects (18 lesions) had no major protocol deviations (the PP population).
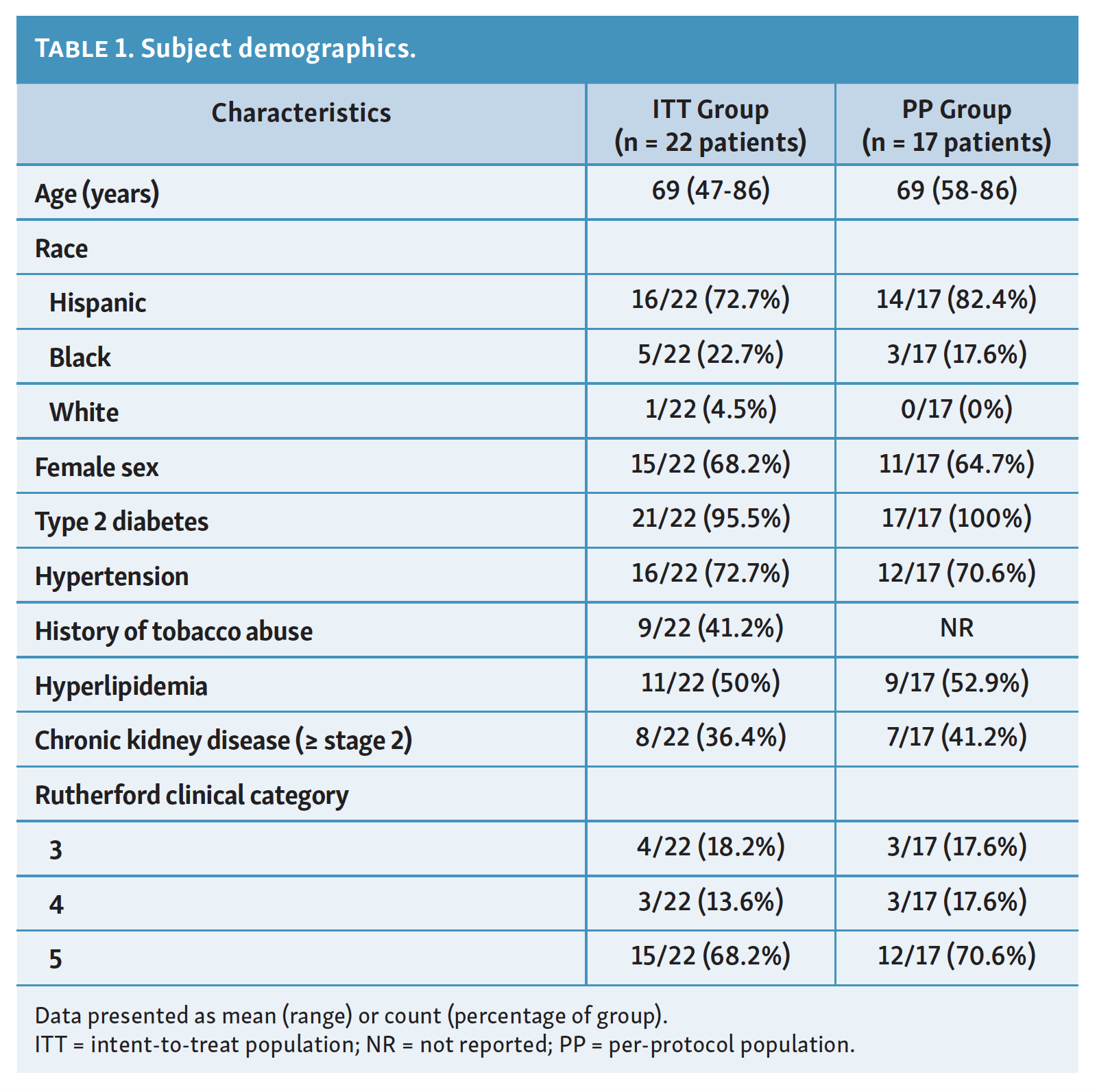
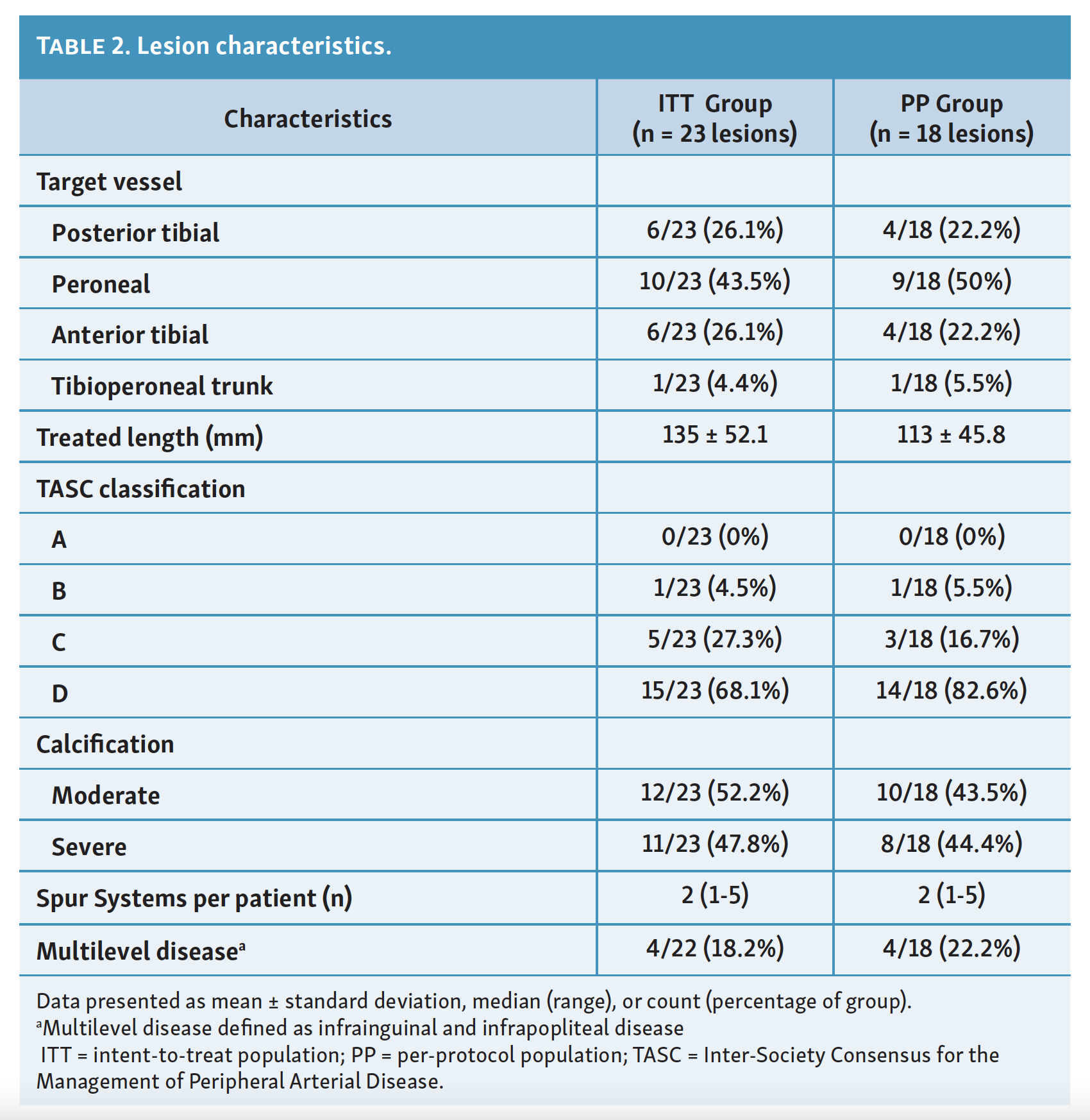
Demographic data are described in Table 1. There was no significant difference in outcomes based on sex, race/ethnicity, or comorbidities. Lesion characteristics are described in Table 2. Treated lesions were located most frequently in the peroneal artery (PP 50%; ITT 43.5%). The mean temporary stent-treated length of the lesions was slightly greater in the ITT population (135 mm) than in the PP population (113 mm). Calcification was classified as mild, moderate, or severe, based on investigator determination by quantitative vascular analysis (QVA). The majority of lesions had moderate or severe calcification, and were classified as TASC level C or D (Inter-Society Consensus for the Management of Peripheral Arterial Disease). Multilevel disease was seen in 22.2% and 18.2% of the PP and ITT groups, respectively.
{kind=link}
{kind=link}
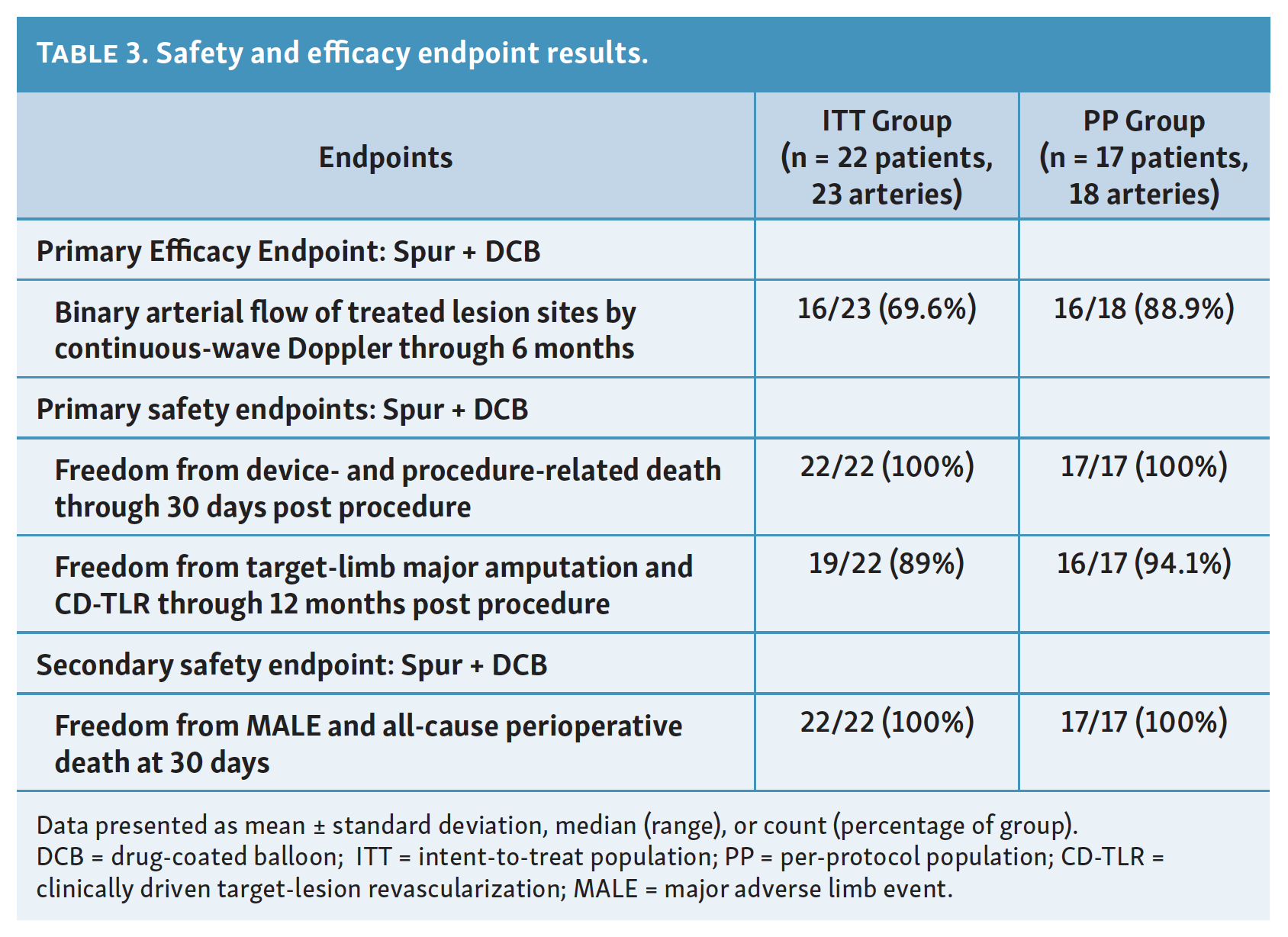
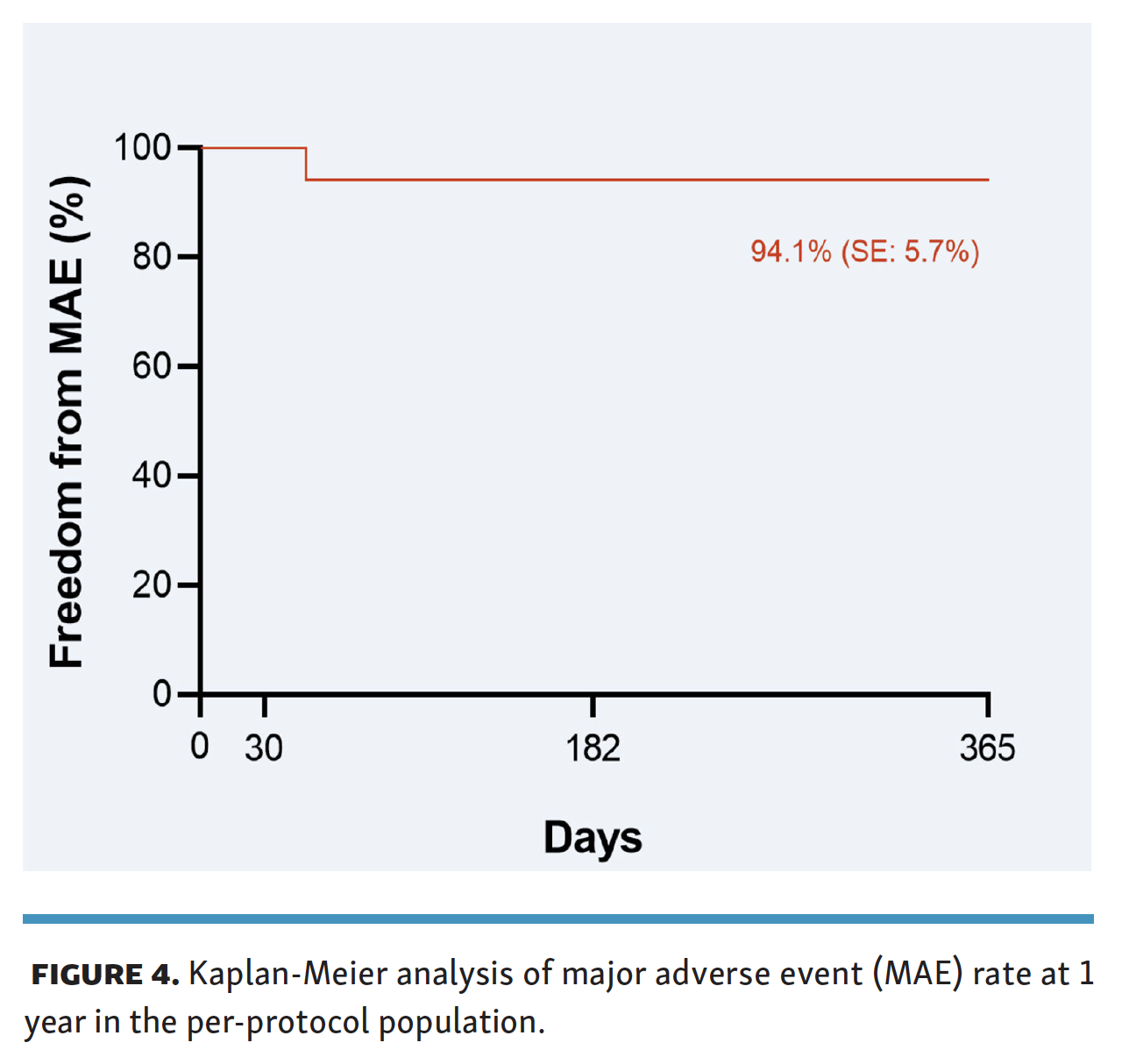
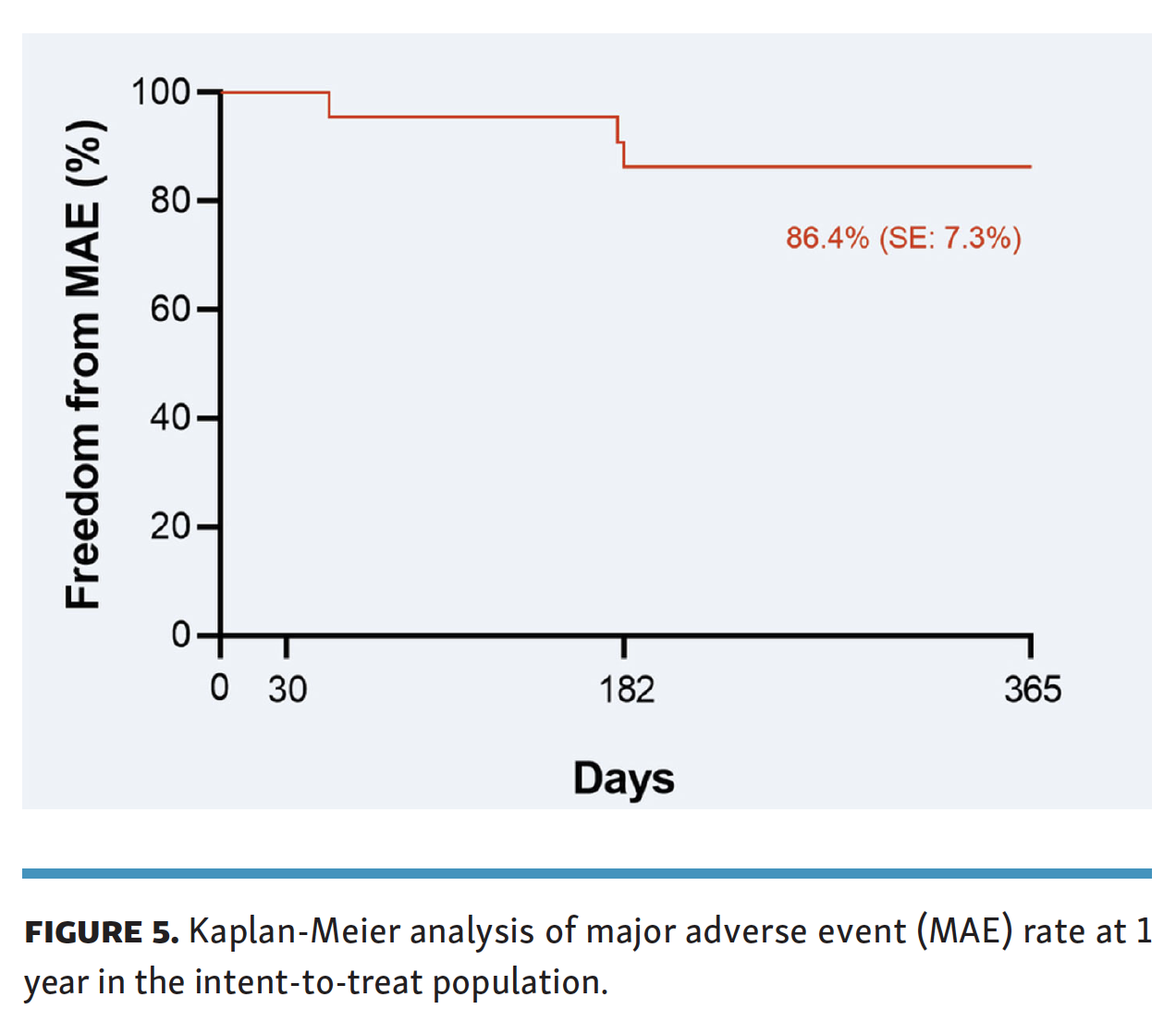
Endpoints. The primary and secondary endpoints are summarized in Table 3. A total of 88.9% (17/18 lesions) and 69.9% (16/23 lesions) of target-lesion sites were patent at 6 months in the PP and ITT groups, respectively (Table 3). The safety analyses showed 0% mortality at 30 days in the PP and ITT populations. The Kaplan-Meier estimate of the safety endpoint of freedom from major adverse events for target-limb MALE or CD-TLR at 12 months was 94.1% (standard error, 5.7%) in the PP group and 86.4% (standard error, 7.3%) in the ITT group (Figure 4 and Figure 5, respectively).
{kind=link}
{kind=link}
{kind=link}
Clinical outcomes. The technical device success rate was 100%. No adverse events were attributed to the investigational device. One procedure-related serious adverse event of severe hypotension occurred during the index procedure, requiring an additional day of hospitalization. Minor procedure-related adverse events included subacute thrombus, vasospasm, type A dissection, vessel perforation caused by a wire, and closure-device malfunction. Adverse events were collected and reviewed by the investigators at each follow-up visit.
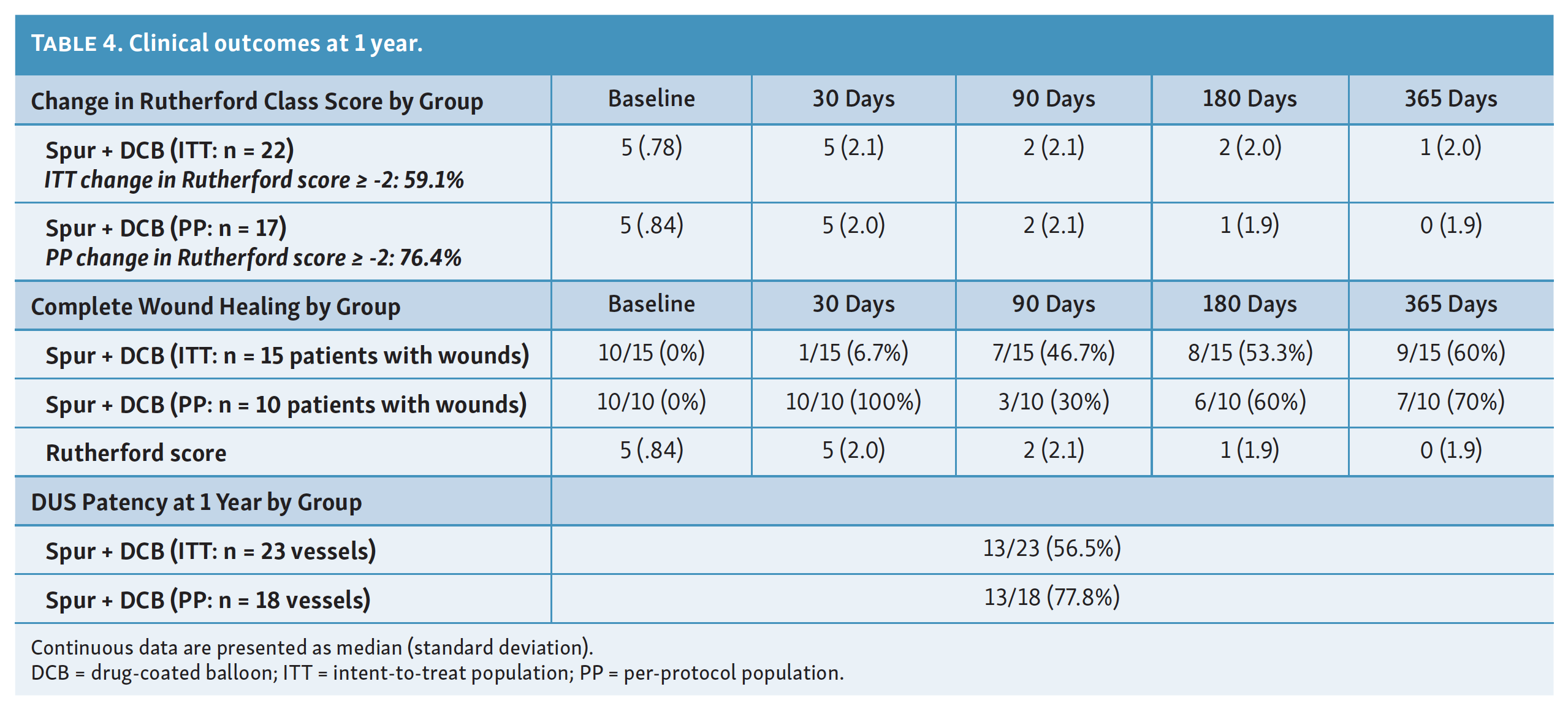
The majority of subjects in this trial experienced an improvement in clinical outcomes, with an average decrease in Rutherford class score by 2 classes (maximum -5, minimum 0) at 12 months, and complete wound healing for >60% of subjects in both the PP and ITT groups (Table 4). A total of 13/18 lesions (77.8%) were patent by DUS in the PP population at 1 year (Table 4).
{kind=link}
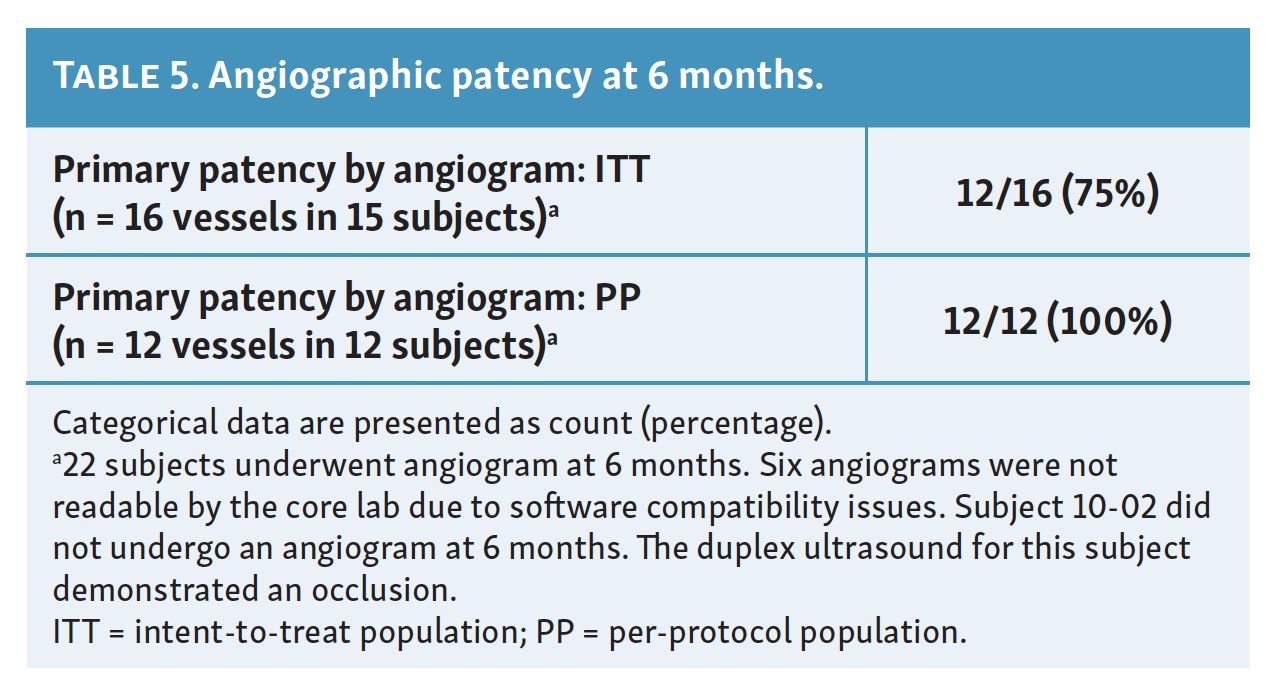
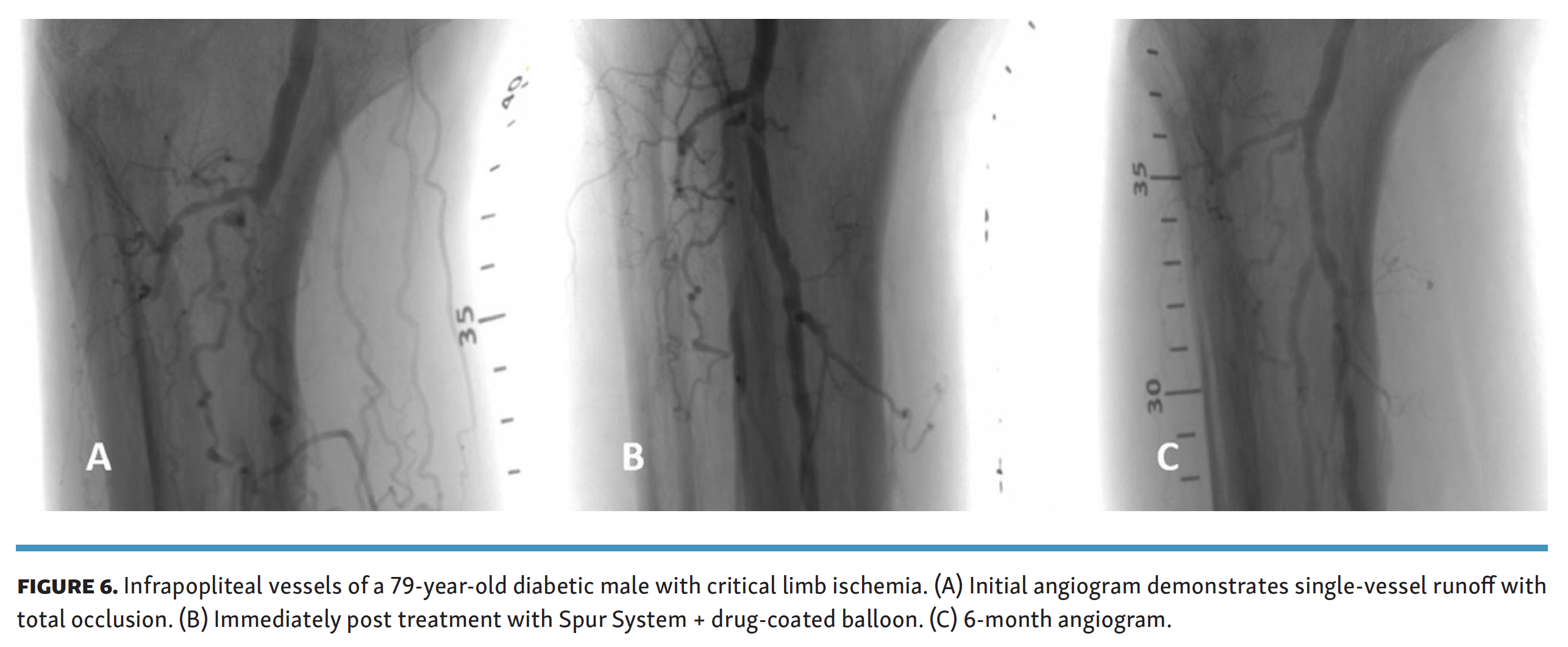
Angiographic data and change in vessel diameter. The results of 6-month angiography are summarized in Table 5. Of the 22 subjects treated with temporary stent + DCB, 21 underwent angiography at 6 months. One subject who was included in both the ITT and PP groups was excluded from angiography, as the patient had already undergone a failed TLR, and DUS revealed a totally occluded index vessel, without change in clinical symptoms warranting another revascularization procedure. Six angiograms were not readable by the core lab due to software issues with the angiogram collection. Patency in the readable angiograms was 12/12 (100%) in the PP group, and 12/16 (75%) in the PP group. Figure 6 demonstrates a treated lesion before treatment, after treatment, and at 6 months.
{kind=link}
{kind=link}
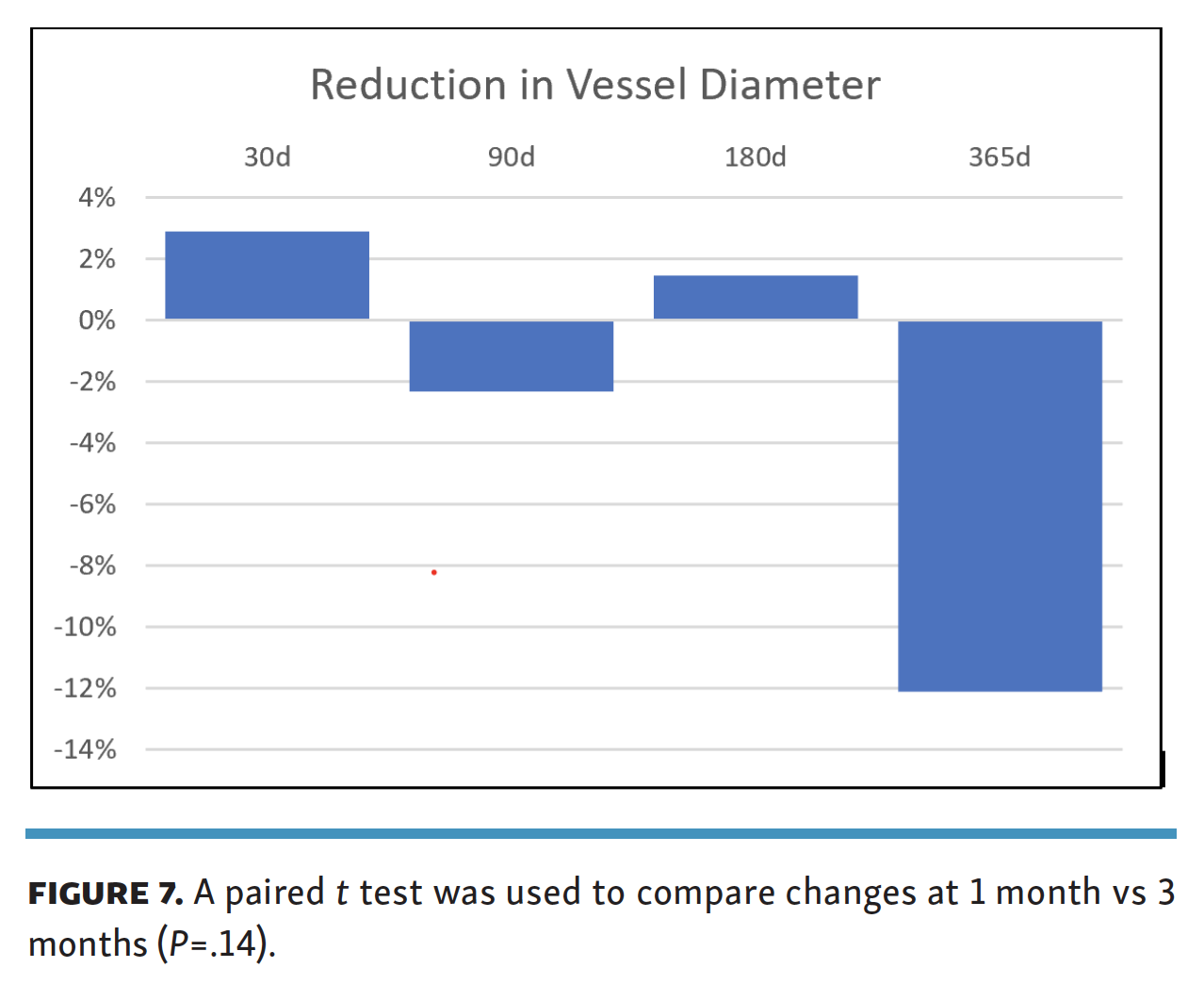
Changes in vessel diameter measured by DUS were captured during follow-up. The vessel diameter was measured at the treated segment, as measured by a ruler based on the initial angiographic measurements, at each time point. These diameter measurements were compared for change across time points. A paired t test was used to compare changes at 1 and 3 months (Figure 7). A statistically significant difference between the time points was not demonstrated (P=.14).
{kind=link}
Discussion
The DEEPER first-in-human trial is the first clinical trial evaluating the safety and performance of a novel technology, the Temporary Spur Stent System. Six-month patency rates were 69.6% in the ITT group and 88.9% in the PP group. These results may suggest patency with this device is positive in comparison with previous DCB trials to date, although these are not directly comparable due to differences in patency endpoints, sample size, and methods.13-17 These patency results remain less satisfactory when compared with drug-eluting stent trials, all of which had short lesion lengths (mean, 17 mm-31 mm), compared with an average lesion length of 113 mm (PP group) in the DEEPER trial.8,18
Subjects treated with the temporary stent experienced improvement in clinical outcomes over the course of 1-year follow-up, including complete wound healing (ITT 60%; PP 70%), and improvement in Rutherford class score >2 (ITT 59.1%; PP 76.4%).
No subjects were lost to follow-up; all subjects were able to be evaluated for safety over the course of 12 months of follow-up. No adverse events were unexpected, and none were determined to be caused by the device. In the temporary stent + DCB-treated PP group, CD-TLR and major amputation rates were 5.6% and 0% at 1 year, and in the ITT group were 13.6% and 4.5% at 1 year, which is consistent with results of other trials of infrapopliteal balloons and stents.8,13-18
Implications for future investigations. This trial provides promising results for further research into the application of the temporary stent in conjunction with a DCB for the treatment of PAD in the infrapopliteal arteries. Large, multicenter, randomized trials should be conducted to provide comparative evidence to assess the efficacy of the temporary stent. In this clinical trial, the Lutonix .014˝ below-the-knee DCB was used due to availability; however, it would be beneficial to observe differences among results with various DCBs. In addition, the temporary stent is drug-agnostic, which may be advantageous given the recent controversy over long-term mortality rates associated with the use of paclitaxel-coated balloons in the femoropopliteal and infrapopliteal arteries.19,20
In addition to the standard outcomes evaluated in this trial, change in vessel diameter was examined in a small group of subjects by calculating the change in vessel diameter from 24 hours post procedure to 12 months post procedure, as measured by DUS. This has not been previously reported in a trial evaluating the performance of a device for treatment of infrapopliteal lesions. A similar phenomenon was recognized in the superficial femoral arteries, where luminal gain was demonstrated in segments treated with DCB.21,22 The luminal gain seen with the temporary stent and DCB may be related to a more efficacious drug transfer in addition to the reduction of acute recoil.
The findings of this study may be indicative of a change in drug uptake in the vessel wall due to facilitated drug delivery. Paclitaxel release from a polymer reservoir has been demonstrated to increase over the course of 28 days after deposition, and then decrease over 180 days.23 The lack of acute luminal loss at 30 and 90 days may indicate that deeper penetration of paclitaxel prevents late lumen loss. The inhibition of vessel recoil may improve sustained drug delivery, even through a calcified vessel wall, thus enhancing the effect of drug on neointimal hyperplasia. Such acute luminal gain may enhance the sustainability of arterial wall contraction to deliver a high volume of blood to the target foot vessels, rapidly delivering oxygenated blood to contribute to wound healing. Further research must be performed to support this idea.
Another unique aspect of this trial was that ultrasound was the modality of measurement for the primary endpoint of patency. Previous studies evaluating the correlation of angiography and DUS in the infrapopliteal arteries have had mixed results. One found that the overall sensitivity/specificity of ultrasound detection of tibial artery patency, compared to angiography, is 93% and 40%, respectively (P<.05);23 however, another study found no correlation between the two modalities.24 Duplex ultrasound is increasingly being used to evaluate the presence or absence of flow in clinical trials of subjects with infrapopliteal disease, as part of a composite endpoint with CD-TLR and amputation.25-27 Due to the small sample size, broad conclusions regarding the use of ultrasound versus angiography in this study are not possible, however, core-lab adjudication of patency for subjects who underwent both ultrasound and angiography at 6 months correlated in this study.
Further device development may involve an integral balloon system and the addition of a drug-coating directly to the device. This would allow for penetration of the arterial internal elastic lamina and deeper antiproliferative drug delivery in one step.
Study limitations. This was a nonrandomized feasibility study intended primarily to examine the short-term safety of the temporary stent. One limitation of this trial is the small sample size. Thus, broad conclusions regarding the efficacy of the temporary stent cannot be drawn. In addition, there was no comparison group for performance.
Inclusion and exclusion criteria may have impacted trial results. Rutherford class 3 (ITT 18.2%; PP 16.7%) subjects were included in the cohort; therefore, not all subjects had critical limb ischemia. At the time of protocol development, a large, ongoing DCB trial in the infrapopliteal arteries permitted subjects with Rutherford class 3 as well; this was permitted in this trial due to this precedent.14 In addition, there were deviations from the angiographic criteria observed in 5 subjects, which significantly impacted the ITT results. This underscores the importance of closely following protocol guidelines in clinical trials.
Further limitations include treatment by a single investigator. It is possible that the use of a single investigator with a limited number of treatment centers may suggest promising data, which may not be replicated in a larger trial. This effect was demonstrated in the DEBATE-BTK, INPACT Amphirion, and IN.PACT DEEP trials, in which the data generated by the single-site trials, DEBATE-BTK and INPACT Amphirion, was not replicated in IN.PACT DEEP.13,15,16 Additionally, follow-up DUS evaluation was performed by a single registered vascular technologist, providing for consistency in follow-up imaging that is not feasible in a large, multicenter clinical trial.
Conclusion
Results of this small feasibility study suggest the temporary stent is safe for the use of treatment of infrapopliteal PAD and CLI. A positive trend in patency was demonstrated, with improvement in clinical outcomes from baseline. Larger, multicenter, randomized trials should be conducted to evaluate further evaluate the safety and efficacy of this device, with special attention given to the unique ability of the temporary stent to contribute to prevention of vessel recoil, while leaving nothing behind in the body.
Disclosures
From 1Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, Michigan; 2The National Institute of Diabetes, Endocrinology, and Nutrition (INDEN), Dominican Republic; 3Department of Cardiology and Vascular Medicine, Grand Rapids, Michigan; 4Interventional Radiology Service, Centro Vascolare Ticino, Inselspital, Universitätsspital Bern, Universitätsinstitut für Diagnostische, Interventionelle und Pädiatrische Radiologie, Bern; 5Interventional Radiology, Auckland City Hospital, Professor of Radiology, University of Auckland, Auckland; 6Reflow Medical, San Clemente, California.
Funding: The study was funded by Reflow Medical.
Clinical trial registration: https://clinicaltrials.gov. Unique identifier: NCT03669458
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. One or more of the authors has disclosed a potential conflict of interest regarding the content herein. The remaining authors report no conflicts of interest regarding the content herein.
The authors report that patient consent was provided for publication of the images used herein.
Manuscript accepted August 10, 2022.
Address for correspondence: Jihad Mustapha, MD, Advanced Cardiac & Vascular Centers for Amputation Prevention, 1525 E. Beltline Ave, NE, Suite 101, Grand Rapids, MI 49503. Email: jmustapha@acvcenters.com