Preoperative C-Reactive Protein Levels Predict Readmission Following Elective Vascular Surgery
Asrar Khan, MD1,2; Derrick L. Green, MD, MBA3; Steve Santilli, MD, PhD, MBA3; Debra K. Johnson, RN1,2; Selma Carlson, MD1,2; Mackenzi Mbai, MD1,2; Rosemary F. Kelly, MD4; Amy A. Gravely, MS5; Brad Bart, MD1,2; Selcuk Adabag, MD1,2; Santiago Garcia, MD6; Qun Chen, PhD7,8; Ion S. Jovin, MD7,8; Edward Lesnefsky, MD7,8; Edward O. McFalls, MD, PhD1,2
ISSN: 2694-3026
J CRIT LIMB ISCHEM 2022;2(2):E39-E44. Epub 2022 May 17.
Abstract
Background. C-reactive protein (CRP) levels may be reduced with long-term administration of ubiquinone (CoQ10) in patients with chronic ischemic heart disease, but the impact of a short-term period of administration in patients undergoing elective vascular surgery is uncertain. Methods. A double-blind, randomized, controlled trial was implemented to determine whether preoperative administration of CoQ10 could reduce cardiac biomarker elevations. Patients were randomly assigned to CoQ10 (400 mg per day) versus placebo for 3 days prior to surgery. B-type natriuretic peptide (BNP), troponin, and CRP levels were obtained before and after surgery. The primary endpoint was peak biomarker elevations and secondary endpoints were length of stay and readmission. Results. A total of 123 patients were randomly assigned to CoQ10 (n = 62) or placebo (n = 61) for 3 days before surgery. At 24 hours post surgery, the group receiving CoQ10 had lower BNP levels, with no intergroup differences in CRP. Within 1 year post discharge, 36 patients (29%) were readmitted and preoperative risk for readmission included diabetes mellitus (hazard ratio [HR], 3.60; 95% confidence interval [CI], 1.46-8.91), active smoking (HR, 3.55; 95% CI, 1.43-8.78), and CRP (HR, 1.35; 95% CI, 1.04-1.76). C-index for all 3 variables predicting readmission was 0.727. Conclusions. Short-term administration of CoQ10 reduced perioperative BNP, but not CRP levels. CRP, along with diabetes and active smoking, were independent predictors of readmission and might be suitable variables to modify as a means of reducing subsequent rehospitalizations following elective vascular procedures.
J CRIT LIMB ISCHEM 2022;2(2):E39-E44. Epub 2022 May 17.
Key words: BNP, C-reactive protein, diabetes mellitus, readmissions, ubiquinone, vascular surgery
Introduction
Among Medicare beneficiaries undergoing vascular surgery, nearly 1 in 4 patients are readmitted within 30 days of hospital discharge and as a diagnosis-related group (DRG), cause of readmission is second only to congestive heart failure.1 Although readmissions following vascular surgery are often unplanned,2,3 identifiable clinical risk factors can be recognized at the time of discharge and include age, socioeconomic factors, and select comorbidities.4-9 There is emerging interest in exploring the utility of perioperative biomarkers as a means of predicting those patients who have the highest risk of adverse postoperative outcomes, including unplanned readmissions.10 Preoperative N-terminal prohormone B-type natriuretic peptide (NT-proBNP) has been recommended as an optimal means of risk stratifying patients undergoing noncardiac operations11 and has value in patients undergoing vascular surgery.12 In support of those studies, we have shown that preoperative NT-proBNP levels predict postoperative risk of myocardial injury.13 C-reactive protein (CRP), a readily available biomarker, can also predict poor outcomes in patients with ischemic heart disease14,15 and together with BNP, may have value in predicting adverse events in patients with vascular disease.16,17
Ubiquinone (CoQ10) is an endogenous antioxidant that improves outcomes in patients with heart failure and ischemic heart disease.18 Reducing oxidant stress in the mitochondria within the myocyte may play a key role in attenuating inflammation within cardiac tissue. In fact, in a meta-analysis, CoQ10 administration significantly decreased plasma CRP levels.19 Interleukin-6 (IL-6) is a secondary messenger cytokine that induces hepatic CRP production20 and is also lowered by administration of CoQ10.21 To no surprise, the greatest effect on CRP reduction with CoQ10 administration is among those patients with elevated IL-6 levels.22 A plausible mechanism for CoQ10’s antioxidant effect on reduced inflammation is the inhibition of IL-6, which is upstream from the production of proinflammatory cytokines.23
In the present study, we assessed the utility of CRP levels in predicting risk of readmission to the hospital following hospital discharge. Because long-term administration of CoQ10 has been shown to reduce CRP levels in selected patients,24,25 testing the effects of a short-term period of administration on postoperative CRP levels is relevant.
Methods
The Human Studies subcommittee of the Research and Development committee at the Minneapolis VA Medical Center approved this study. All patients were screened at their preoperative vascular clinic within 4 weeks of a scheduled operation. Inclusion criteria for eligible patients was a clinical indication for an elective vascular operation. Exclusion criteria included emergent or urgent need for vascular surgery, known allergic reaction to CoQ10, or participation in another research project. Individuals who met the inclusion and exclusion criteria were offered participation in the trial and given informed consent. The design was a double-blind, randomized, controlled trial.
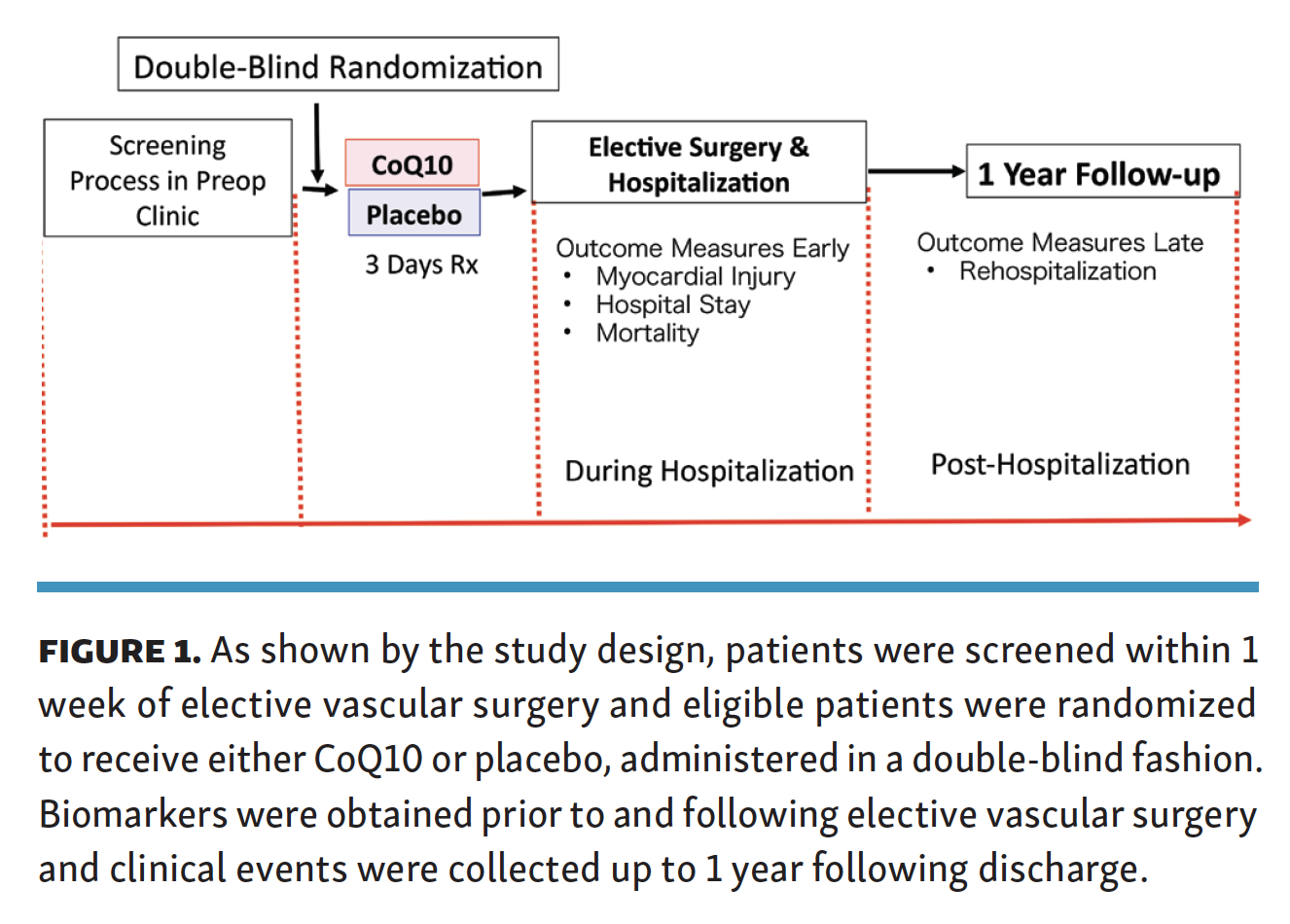
Randomization and assignment of treatment. The methodology of the primary trial results has been previously published13 and is summarized in Figure 1. Following informed consent, patients were referred to a research pharmacist and treatment was randomly designated in a blinded fashion, with permuted blocks. Tablets of either CoQ10 or placebo were prepared according to assigned treatment without medication identifiers. The prepared medication was provided to the patients by pharmacy, with instructions to take 2 tablets per day for 3 days prior to surgery. The rationale for 3 days of therapy relates to the logistics of when patients are seen prior to their elective procedure and the feasibility of executing a trial within the time frame of the operation. The dose of 400 mg per day was chosen based on prior clinical studies and the observation that plasma levels peak at 6 hours and remain increased for 33 hours.26 The research coordinator confirmed that patients took all medications as prescribed. The research coordinator followed the patients throughout the hospitalization period and recorded clinical events within 1 year following discharge.
{kind=link}

Elective surgery and outcomes. Patients were admitted to the surgical floor, either the night before or the day of the surgery. In the entire study cohort, preoperative symptoms involved carotid disease (n = 35), lower-extremity arterial occlusive disease (n = 63), and an expanding aortic aneurysm (n = 37). Procedures performed included carotid endarterectomy (n = 36), infrainguinal bypass procedure (n = 78), and open intra-abdominal procedures (n = 9), and there were no intergroup differences in either the clinical symptoms or vascular procedures.
Blood was obtained for baseline preoperative cardiac biomarkers, including NT-proBNP, troponin I, and high-sensitivity CRP and repeated daily at 24 hours and 48 hours if the patient remained in the hospital. NT-proBNP and troponin I levels were considered abnormal if they exceeded the upper reference limit (URL) of the specific assay. Management of the patients was done by the surgical team, and consultative cardiologists, as needed, without any knowledge of assigned treatment. No cases were cancelled or delayed because of abnormal cardiac biomarker measurements. Blood was obtained from each patient for the analysis of troponin I, CRP, and NT-proBNP. Baseline lab was obtained either on the morning of the surgery, or the night before if the patient was lodging. The research coordinator confirmed that each subject had taken their assigned drugs for the 3 days prior to the operation. Blood assays were repeated each day following the operation for up to 48 hours. The URL of each assay was used, based on the manufacture’s guidelines for that specific assay. The primary endpoint measure was NT-proBNP level at 24 hours following surgery.13 In this article, we have focused on clinical variables that predicted a secondary endpoint measure, which was readmission within 1 year following hospital discharge.
Statistical analysis. Data are expressed as either mean ± standard deviation or median with interquartile range (IQR) when specified. All clinical variables were obtained, including biomarker levels at baseline and following surgery. Biomarker levels were also expressed as exceeding the URL of each specific assay and categorized as the incidence of elevated values. Intergroup differences between patients randomized to CoQ10 versus placebo were tested by Student’s t test, with significance set at the P<.05 level for comparing continuous variables. For categorical variables, Chi-square tests were utilized. Among data that were not normally distributed, nonparametric testing was performed to confirm the findings using a Wilcoxon 2 sample test. Readmissions to the hospital were categorized according to diagnoses and time from discharge. All clinical variables were compared between those patients with and without readmissions. A multivariate logistic regression model was then done, entering all univariate variables that had a P≤.10 into the model to determine independent predictors of readmission. Nonsignificant variables were discarded and left 3 clinical variables that predicted readmission.
Results
Among all patients, preoperative cardiac risks included a history of ischemic heart disease (n = 52), congestive heart failure (n = 12), stroke (n = 23), and diabetes mellitus (n = 48); the planned vascular procedures were infrainguinal (n = 78), carotid (n = 36), and intra-abdominal (n = 9). There were no intergroup differences in these clinical variables according to the assigned treatment. At 24 hours following surgery, median NT-proBNP levels in the treatment and placebo groups were 397 pg/mL (IQR, 211-686) and 591 pg/mL (IQR, 288-1433), respectively (P<.01), while median CRP levels were 21 mg% (IQR, 12-40) and 20 mg% (IQR, 10-41), respectively (P=.83). Peak median postoperative troponin I levels were 0.040 ng/mL (IQR, 0.024-0.111) in the CoQ10 group and 0.052 ng/mL (IQR, 0.029-0.141) in the placebo group (P=.19). During the hospitalization, there were no in-hospital deaths and a postoperative myocardial infarction was diagnosed in 4 patients (2 patients from the CoQ10 group and 2 patients from the placebo group). Total length of stay was 3.05 ± 3.17 days in the CoQ10 group and 3.71 ± 3.74 days in the placebo group (P=.29).
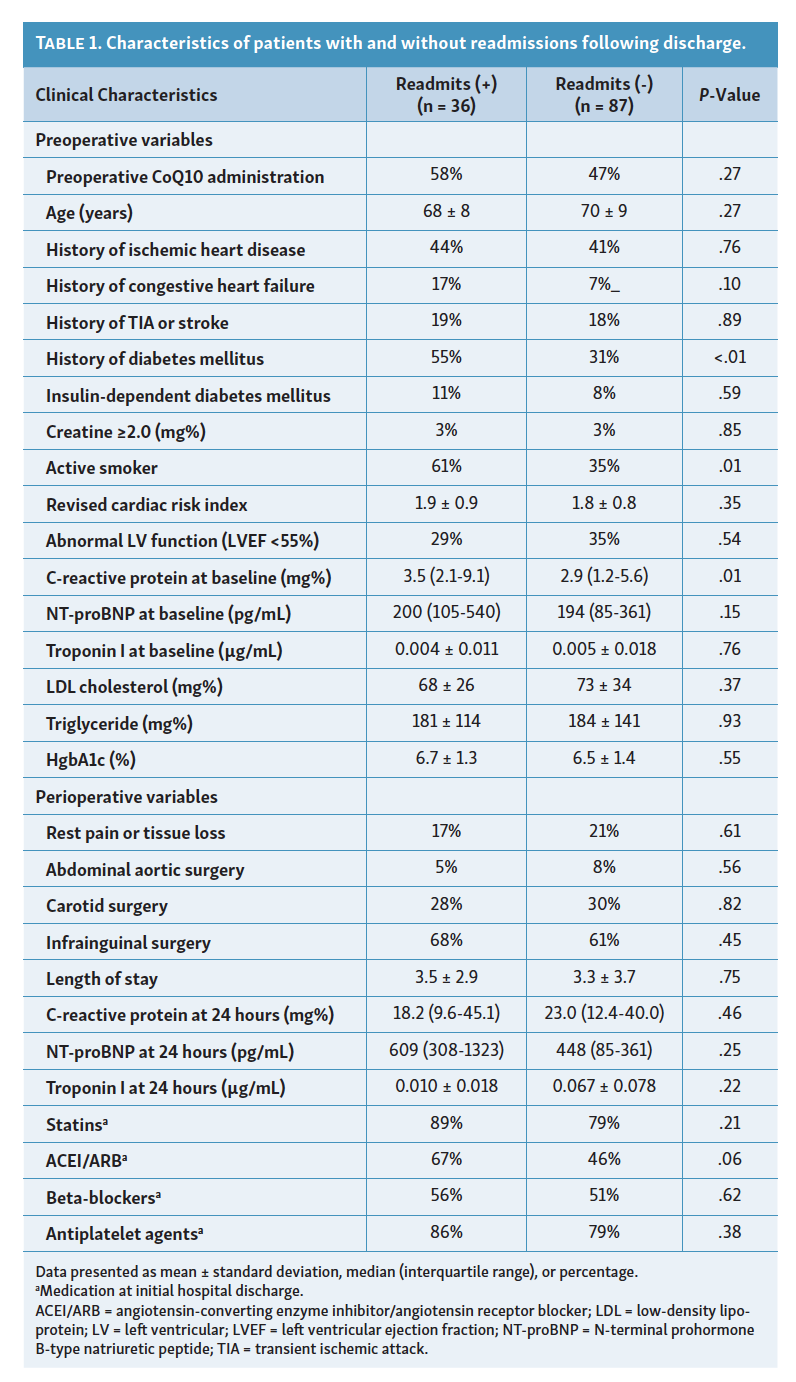
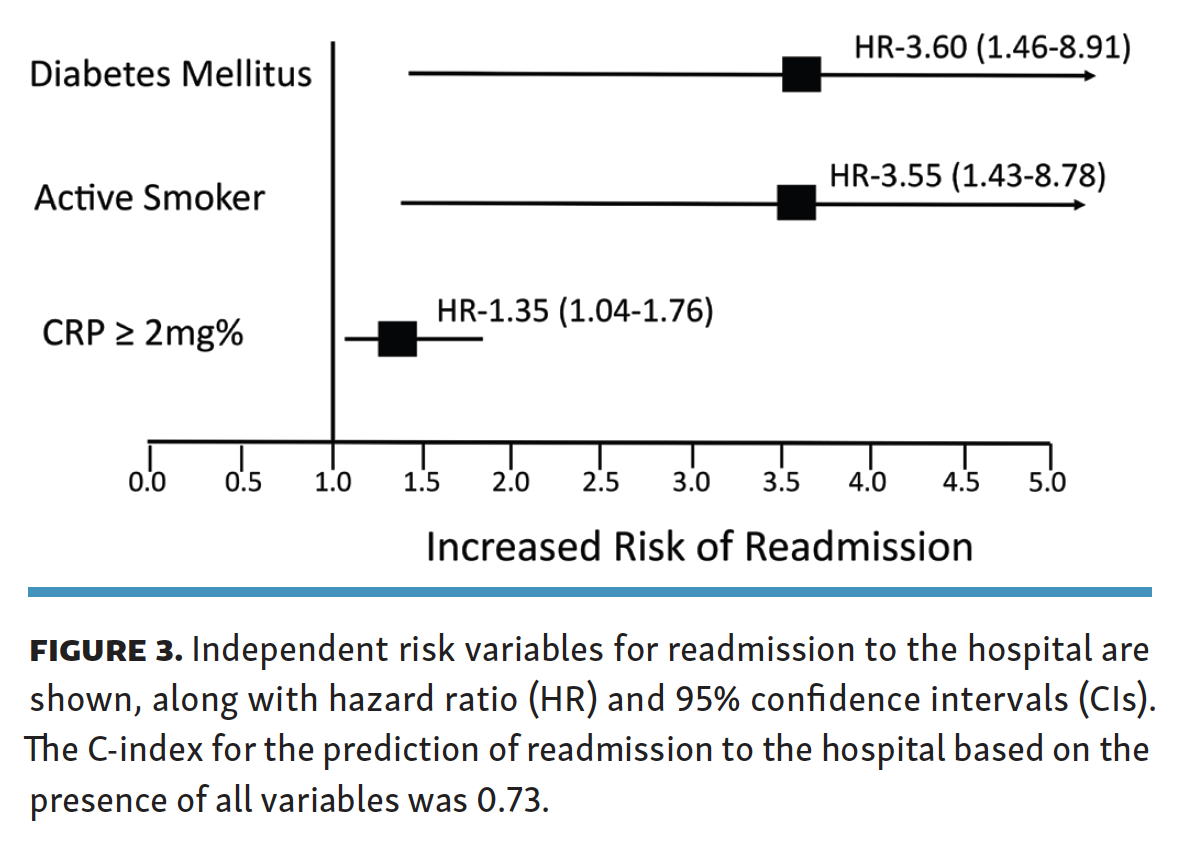
Thirty-six patients (29%) were readmitted to the hospital within 1 year of hospital discharge following their elective surgery. The diagnosis at the time of readmission was related to an infection in 13 patients, 9 of which occurred within 30 days of the original hospital discharge (Figure 2). Table 1 shows the bivariate relationships for clinical variables in patients with univariate predictors for readmission to the hospital and Figure 3 shows the independent risks produced from a multivariate logistic regression model. This model was shaved down twice—once by only taking bivariate predictors with a P-value of ≤.10 and then subsequently removing variables that were not significant, leaving diabetes mellitus (hazard ratio [HR], 3.60; 95% confidence interval [CI], 1.46-8.91), active smoking (HR, 3.55; 95% CI, 1.43-8.78), and elevated preoperative CRP (HR, 1.35; 95% CI, 1.04-1.76). C-index for all 3 variables predicting readmission was 0.727.
{kind=link}
{kind=link}
{kind=link}



Discussion
The principal finding of the present study is that baseline CRP levels prior to elective vascular surgery were a strong predictor of readmission to the hospital within 1 year of hospital discharge. Along with diabetes and active smoking, CRP was an independent predictor of readmission and each of these variables might be worth targeting with additional interventions preoperatively. Although short-term preoperative administration of CoQ10 did not reduce CRP levels in the present study, it did reduce postoperative NT-proBNP levels.13 Prior studies have advocated for the use of BNP as a preoperative clinical risk variable11,12 and may justify larger studies to test whether a longer period of treatment, which can lower BNP and possibly CRP, might reduce clinically meaningful adverse outcomes.
Readmission rates have been deemed an important measure of quality of care. As part of the Affordable Care Act from 2010, the center for Medicare and Medicaid Services has developed new policies to reduce readmissions to the hospital. Among Medicare beneficiaries undergoing vascular surgery, 24% were readmitted within 30 days of hospital discharge, which was second only to congestive heart failure as the most common DRG cause of readmission.1 We have looked at ways of reducing readmissions among patients who were discharged from the hospital following a myocardial infarction, and have found that some patients might be better screened in the emergency room.27 Readmissions following vascular surgery are often unplanned,2,3 with identifiable risks at the time of discharge that include age, chronic illnesses, socioeconomic factors, and chronic limb ischemia.4-8 Although our cohort of patients undergoing elective vascular surgery was a heterogeneous group, all of the patients were scheduled for elective procedures and for that reason, had stable, non-urgent presentations. In fact, the patients were screened within 1 week of the procedure and after giving consent, were provided with the tablets to take for 3 days prior to surgery. The study protocol was focused on the characterization of biomarkers prior to and following surgery and our goal was to test whether preoperative administration of CoQ10 could lower the biomarkers following surgery. NT-proBNP levels are an important predictor of perioperative risk in patients undergoing noncardiac surgery and our study not only supports that contention, but shows that BNP levels can be lowered with preoperative administration of CoQ10.13 CRP levels, however, were not different between the treatment and placebo groups, suggesting that additional interventions might be needed to reduce either oxidant stress or nonspecific inflammatory marker elevations following surgery.
Among patients presenting with an acute coronary syndrome and undergoing coronary interventions, preprocedural CRP is an independent predictor of readmission to the hospital within 6 months of hospital discharge.10,28 Clearly, targeting inflammation as a way of improving outcomes in patients with cardiovascular diseases is an important initiative.14 In fact, among patients with a recent myocardial infarction and an elevated high-sensitivity CRP (≥2.0 mg%), the CANTOS (Canakinumab Anti-inflammatory Thrombosis Outcomes Study) trial demonstrated that inhibition of interleukin-1β (IL-1β) reduces the composite of adverse vascular events and mortality.29 Canakinumab is a monoclonal antibody that inhibits the release of CRP by blocking IL-1β and the subsequent release of IL-6.30 Among consecutive hospitalized patients, those with an elevated CRP identify as an increased risk of readmission to the hospital when normalized to albumin ratios and blood glucose levels.16 This underscores the important relationship between nutritional status and the metabolic syndrome that may complicate the early postoperative recovery period with risks of subsequent infections. In support of our observations, an elevated CRP level at baseline prior to cardiac surgery is an important predictor of adverse outcomes following hospital discharge31-33 and among patients undergoing vascular surgery, predicts early graft failure.34 Among large groups of patients with known vascular disease, there is growing awareness that an elevated CRP level is an important identifier of recurrent vascular events, and potentially modifiable with newer, novel anti-inflammatory regimens.35-38
Conclusion
An elevated baseline CRP level in patients undergoing elective vascular surgery is an important biomarker for identifying those patients at increased risk of readmission to the hospital. Additional significant clinical risks for readmission using multivariate regression include diabetes mellitus and active smoking. We have shown that a short period of CoQ10 administration reduced BNP, which is an important predictor of perioperative adverse events. A major unanswered question, however, is whether pharmacologically lowering these biomarkers, which may be a marker of systemic inflammation and sickness, will lead to a reduction in clinically relevant adverse outcome measures. Additional studies should also determine what threshold of biomarker elevation requires such pharmacological interventions as well as whether a longer period of administration of CoQ10 prior to high-risk operations might potentially reduce CRP and risk of readmissions to the hospital following elective vascular surgery.
Affiliations and Disclosures
From the 1Division of Cardiology, Minneapolis VA Medical Center, Minneapolis, Minnesota; 2Division of Cardiology, Department of Medicine, University of Minnesota, Minneapolis, Minnesota; 3Division of Vascular Surgery, Minneapolis VA Medical Center, Minneapolis, Minnesota; 4Division of Cardiothoracic Surgery, University of Minnesota, Minneapolis, Minnesota; 5Department of Research Statistical Center, Minneapolis VA Medical Center, Minneapolis, Minnesota; 6Minneapolis Heart Institute, Minneapolis, Minnesota; 7Department of Medicine, Virginia Commonwealth University, Richmond, Virginia; and the 8Division of Cardiology, McGuire VA Medical Center, Richmond, Virginia.
Clinicaltrials.gov Identifier: NCT03956017
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript accepted May 4, 2022.
Address for correspondence: Edward McFalls, MD, Richmond VAMC, Hunter Holmes McGuire VA Medical Center, 1201 Broad Rock Boulevard, Richmond, VA 23249. Email: mcfal001@umn.edu