Orbital Atherectomy Treatment of Peripheral Artery Disease and Critical Limb Ischemia
Jihad A. Mustapha, MD1; Fadi A. Saab, MD1; Brad J. Martinsen, PhD2; Ann N. Behrens, BS2; Miguel F. Montero-Baker, MD3; Bret N. Wiechmann, MD4; Eric C. Scott, MD5; David G. Armstrong, DPM, MD, PhD6; Nicolas W. Shammas, MD7; George L. Adams, MD8
ISSN: 2694-3026
J CRIT LIMB ISCHEM 2021;1(3):E118-E125. Epub 2021 July 15.
Abstract
Orbital atherectomy (OA), a unique form of atherectomy, utilizes orbital sanding and pulsatile forces to deliver effective treatment of peripheral atherosclerotic lesions with varying levels of occlusion and calcification. This approach to endovascular therapy involves the use of differential sanding to preferentially ablate fibrous, fibrofatty and calcified lesions, while deflecting healthy tissue away from the crown. The eccentrically mounted crown design also allows the device to generate pulsatile forces that may penetrate the medial layer and fracture calcium, resulting in compliance change that facilitates low pressure balloon angioplasty and reduces the need for bailout stenting. The combination of plaque modification, improved vessel compliance, and lumen enlargement via OA can effectively restore blood flow in vessels above- and below-the-knee, relieving symptoms and improving limb salvage rates in patients with peripheral artery disease (PAD) and critical limb ischemia (CLI). Numerous peripheral OA clinical studies have confirmed the high rates of procedural success, freedom-from (FF) major adverse events, and FF major amputation. In addition, economic analyses have also shown the value of OA as a first line endovascular therapy for PAD and CLI. We review here the mechanism of action of OA, supporting clinical study evidence, and corresponding economic analyses.
J CRIT LIMB ISCHEM 2021;1(3):E118-E125. Epub 2021 July 15.
Key words: orbital atherectomy; peripheral artery disease; critical limb ischemia
Review
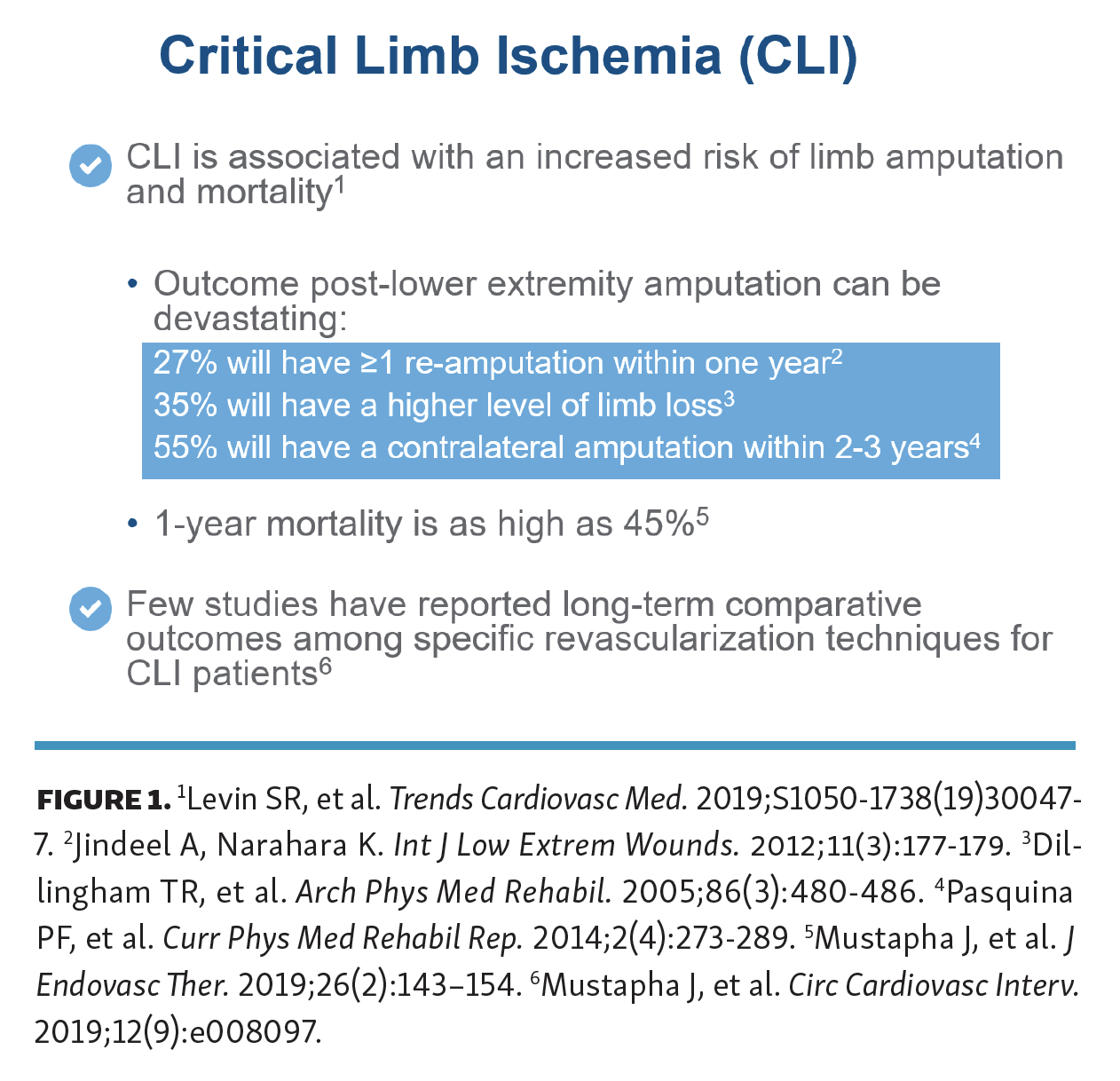
Peripheral artery disease (PAD) is becoming extremely common worldwide, especially as risk factors and independent predictors for PAD rise to pandemic proportions. PAD affects more than 202 million people worldwide, and is prevalent in both high and low income countries.1 Approximately 18 million Americans have PAD and 2 million of these patients suffer from critical limb ischemia (CLI),2,3 the end stage of PAD.4 CLI is highly prevalent in older patients with diabetes and/or end-stage renal disease5 and is associated with high risk of amputation and mortality.6 As shown in Figure 1, the results following lower extremity amputation can be devastating — 27% of these patients will have one or more re-amputation(s) within 1 year,7 35% will have a higher level of limb loss,8 and 55% will have a contralateral limb amputation within 2-3 years.9 Furthermore, the mortality rates after primary amputation are very high, with rates ranging from 9% to 33% at 1 year7,8,10,11 and 26% to 82% at 5 years.7,10–12 Despite such devastating outcomes, primary amputation remains a common treatment modality for CLI.13
{kind=link}

The most severe forms of PAD and CLI often involve heavily calcified lesions which may be more difficult to treat with angioplasty alone. One of the main risk factors for atherosclerotic plaque and vascular calcification is advanced age, since atherosclerotic lesions and calcium increase throughout life.14 Other risk factors include hypercholesterolemia, diabetes, hypertension, and smoking, many of which are on the rise worldwide.1,15 Historical methods of intervention, including balloon angioplasty, may be less effective for treating calcified lesions. These challenging lesions require higher inflation pressure, thus increasing the incidence of plaque rupture, embolization, and dissection.16 Orbital atherectomy (OA; Cardiovascular Systems, Inc.) is a unique device with an eccentrically mounted crown that treats peripheral lesions above-the-knee (ATK) and below-the-knee (BTK) via a dual mechanism of action (MOA): orbital sanding and pulsatile (repeated striking) forces. The orbital sanding removes intimal plaque while the repeated impact of the crown on the vessel wall (pulsatile forces) may fracture medial calcium to further enhance vessel compliance. The safety and efficacy of OA has been shown in numerous clinical studies. This review will cover the MOA of OA, as well as the results of the associated clinical and economic studies.
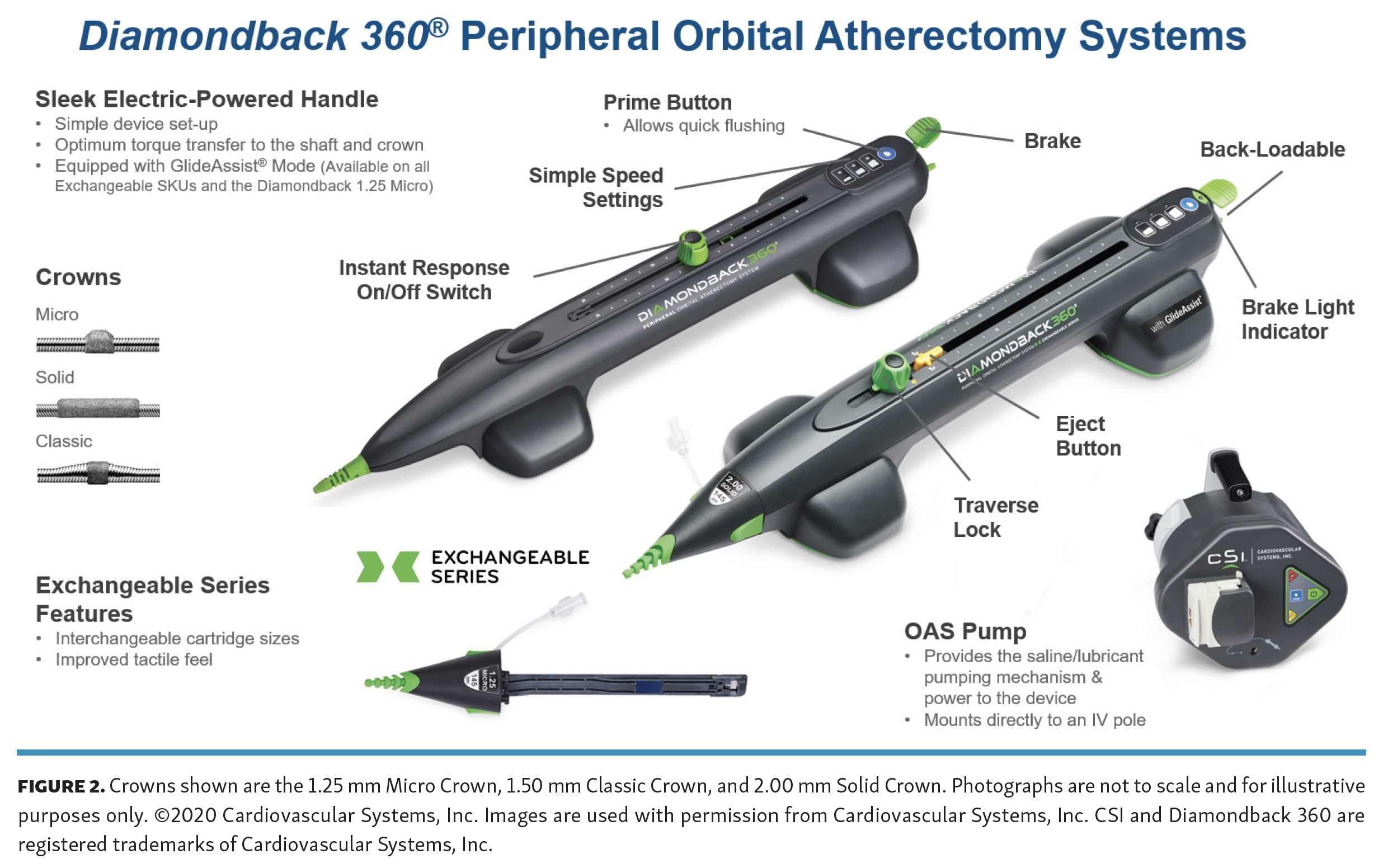
Orbital atherectomy device description and mechanism of action. The Diamondback 360 (Figure 2) and Stealth 360 peripheral orbital atherectomy systems are designed to bi-directionally ablate/sand peripheral intimal plaque and impact deeper calcium in order to restore blood flow and improve vessel compliance in diseased peripheral arteries. The device is designed to track and spin over the ViperWire Advance and ViperWire Advance with Flex Tip guidewires (CSI). OA uses a single-use, low profile catheter attached to an electric handle, allowing for easy control of rotational and directional speed. The control knob mounted on the top of the handle allows the physician to track the catheter forward or backward in a controlled manner. Three speed selections can increase the rotational speed of the crown thereby increasing the orbital curve and ablation efficiency. The crown is available in three styles (classic, solid, and micro) and sizes ranging from 1.25 mm to 2.00 mm; the crown size is selected based on its ability to cross the lesion within the minimum proximal reference vessel diameter at the treatment site. The Diamondback 360 Exchangeable Series allows physicians to use multiple crowns with one handle to treat multilevel disease cases; cartridges are available with various crown size and shaft length configurations. Recently, Mustapha and colleagues published a systematic review with an emphasis on combined inflow and outflow revascularization.17
{kind=link}

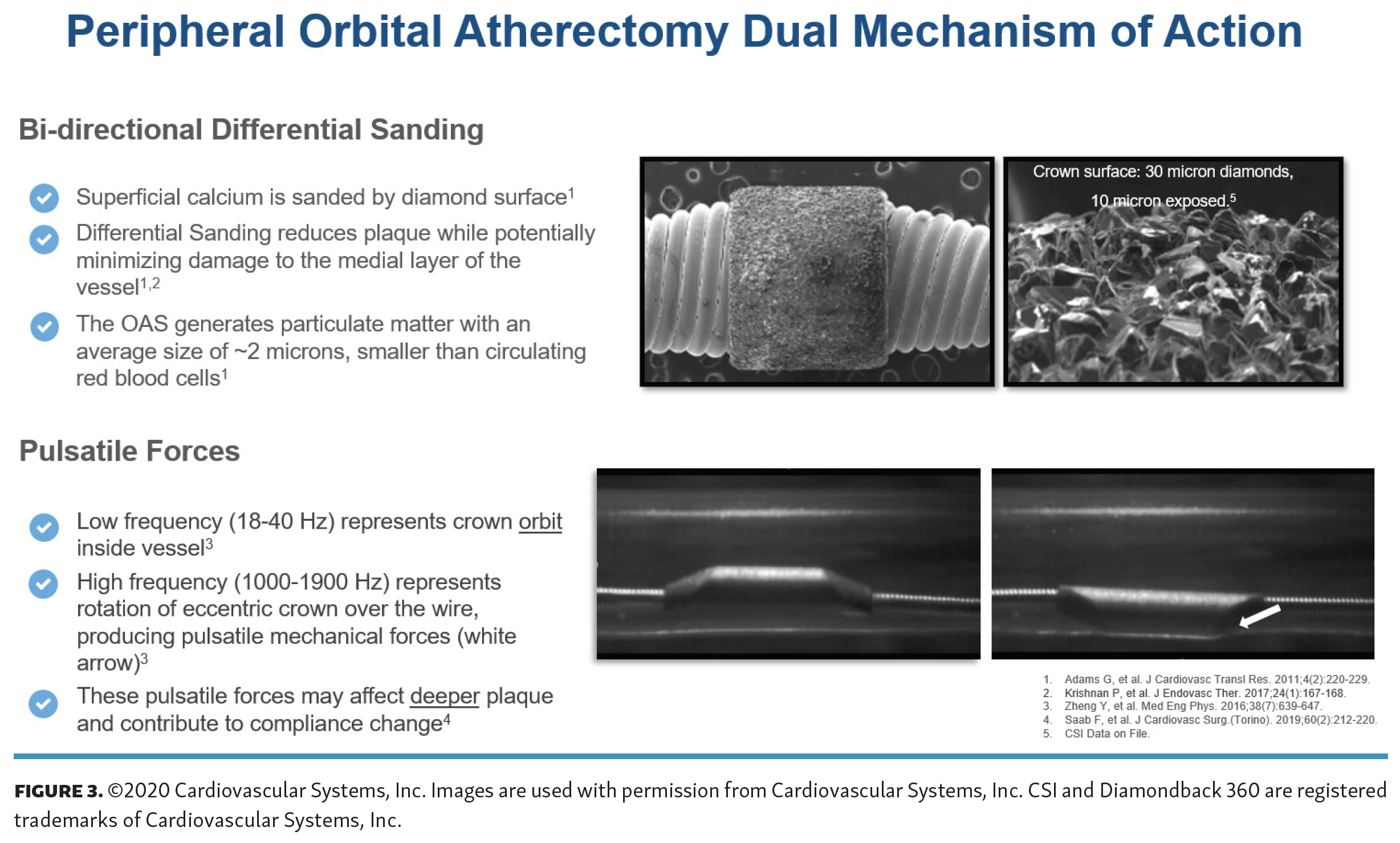
The eccentrically mounted crown is attached to the distal end of the catheter; when the catheter rotates at high speeds, centrifugal force pulls the mass of the crown toward the vessel wall in a circular orbit (Figure 3). The centrifugal force equals the mass of the crown times the square of rotational velocity divided by the radius of the orbit. Since the radius of the orbit is fixed within the confines of an arterial wall, force increases to the second power as velocity increases. Thus, allowing the operator to control the degree of lesion modification, a mode of control not offered by any other form of atherectomy. By changing rotational speed, the operator can change the amount of force exerted on the vessel wall or the effective radius of orbit. Despite the abrasiveness of the crown, intimal damage to the vessel is minimized during the procedure because of a phenomenon called differential sanding. During the operation, the healthy elastic tissue flexes away from the crown, while calcified or fibrous material is engaged by the crown and sanded down. The orbital mechanism allows for continuous flow of blood and saline during treatment, minimizing the risk of thermal damage to the vessel wall which can be a cause of restenosis. The size of particulate generated is generally smaller than a red blood cell and is small enough to be absorbed by the reticuloendothelial system.
{kind=link}

The orbital atherectomy MOA also exerts pulsatile forces via the repeated striking of the crown on the vessel wall (Figure 3; white arrow) as it orbits around the internal surface of the vessel.18 Specifically, as the crown rotates 60,000-140,000 rpm, the offset portion of the crown rhythmically strikes the vessel wall, creating pulsatile energy18 (aka, shockwaves) that may penetrate and impact deeper calcification. These micro-fractures/cracks may further improve the compliance of the vessel, allowing for low-pressure angioplasty while minimizing tissue damage and bailout stenting.
Also, the lesion modification described above may help to improve drug uptake into the vessel wall when drug-coated/eluting technologies are utilized post orbital atherectomy. Briefly, a cadaver study published by Tzafriri et al showed that calcified plaque limited intravascular drug delivery.19 The authors showed that absorption rate varied inversely with pre-treatment calcium scores, and that OA treatment improved diffusivity in the lesion by an average of 70%.
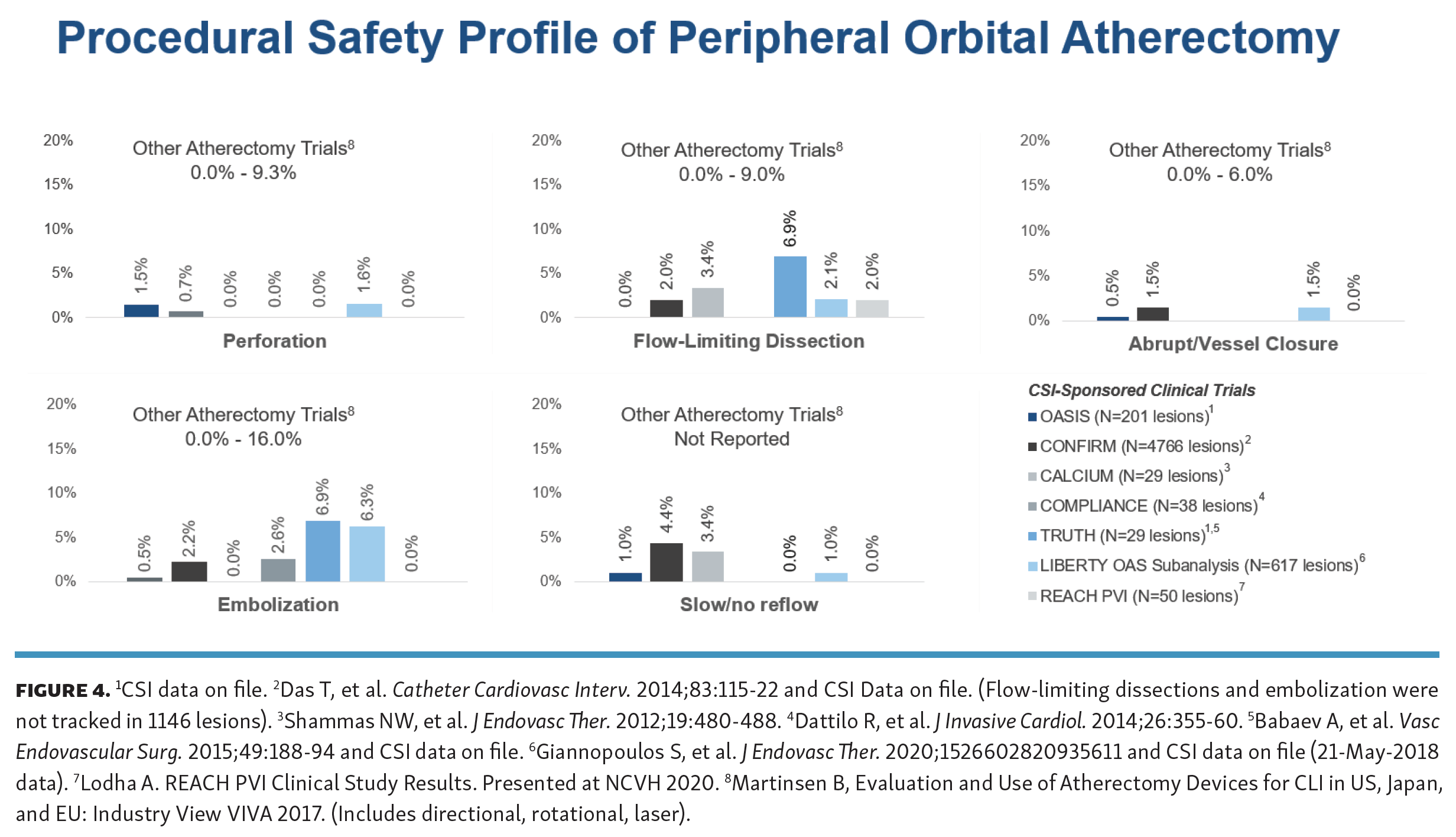
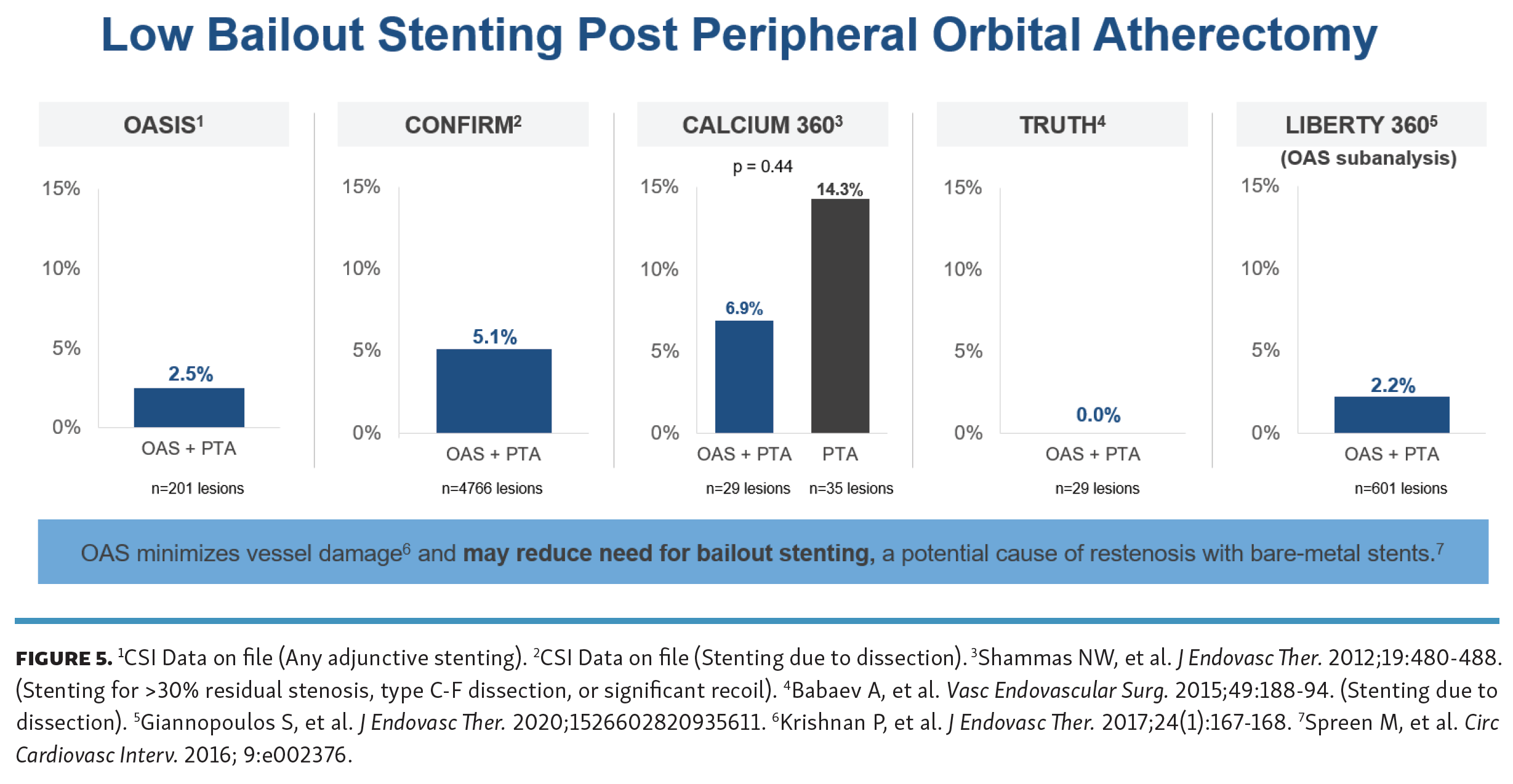
Orbital atherectomy clinical trials and economic analyses. Orbital atherectomy clinical trials have shown that OA minimizes angiographic complications (Figure 4) and vessel damage, reducing the need for bailout stenting (Figure 5), a potential cause of restenosis. Below is a review of the supporting clinical trial data.
{kind=link}
{kind=link}


OASIS Trial. OASIS (Orbital Atherectomy System for the Treatment of Peripheral Vascular StenosIS) was a multicenter, single arm, investigational device exemption trial designed to assess the safety and efficacy of OA for treating chronic infra-popliteal arterial occlusive disease in PAD and CLI patients and enrolled 124 patients.20 The primary safety endpoint was major adverse events (MAE), defined as death, myocardial infarction, amputation, or repeat revascularization, at 30 days and occurred in 3.2%. Procedural success (final diameter stenosis ≤30%) was achieved in 90.1% of cases. At 6 months the MAE rate was 10.4%. The authors of the OASIS study concluded that OA is a safe and unique approach to revascularization of the infrapopliteal arterial circulation in patients with chronic limb ischemia. Short-term data demonstrated substantial symptomatic improvement and infrequent need for further revascularization or amputation.
CONFIRM Registry Series. The purpose of the CONFIRM registry series was to evaluate the use of OA in lower extremity peripheral arteries and to optimize the treatment technique using the device.21 Three peripheral OA device iterations were assessed: CONFIRM I evaluated the use of the Diamondback 360 exclusively (N=733 subjects), CONFIRM II evaluated Predator 360 (N=1127 subjects), and CONFIRM III evaluated Diamondback 360, Predator 360 and Stealth 360 (N=1275 subjects). The only requirement for enrollment was medically necessary treatment in accordance with the OA Instructions for Use. In the study, 35.4% of patients were claudicant Rutherford class three, and 42.7% had critical limb ischemia, Rutherford classes 4-6.21 Overall complication rates were low, the most common was dissection (11.3%). Balloon angioplasty and stenting were used in 73.3% and 5.7% of lesions treated, respectively.Plaque removal was lowest in soft plaques (41%) and highest in severely calcified lesions (54%).21 Interestingly a change in OA treatment strategy was noted over time, including changes in OA run time and crown sizes used. CONFIRM I had a significantly longer OA run time compared to CONFIRM II and III, and the crown sizes used in CONFIRM II and III were smaller than the crowns used in CONFIRM I. Both of these trends corresponded with a downward trend in procedural complications throughout the registry series, including lower rates of slow flow, vessel occlusion and spasm. The authors of the CONFIRM registry series concluded that a change in device usage to shorter spin times and smaller crowns across the study series corresponded to a lower incidence of adverse events (slow flow, vessel closure, and spasm) regardless of calcium burden or co-morbidities. These results suggest that vessel compliance change rather than luminal gain should be the goal of atherectomy.21
CALCIUM 360 Trial. CALCIUM 360 was a prospective, multicenter, randomized controlled trial to evaluate OA with adjunctive balloon angioplasty (BA) vs BA-only for treatment of calcified infrapopliteal lesions in 50 patients with CLI.22 The adjunctive balloon inflation pressure was significantly lower in the OA+BA group (5.9 vs 9.4 atm; P<.001) and use of orbital atherectomy was associated with numerically fewer dissections and lower bail-out stenting.22 Procedural success was numerically higher in the OA+BA group compared to BA-only (93.1% vs 82.4%; P=.27). At 12 months, the OA+BA group had significantly higher freedom from MAE (93.3% vs 57.9%; P=.006) and higher freedom from all-cause mortality (100% vs 68.4%; P=.01); however, freedom from target-vessel revascularization rates were similar (93.3% vs 80.0%; P=.14).22 The authors of the CALCIUM 360 trial concluded that vessel preparation with OA appears to increase the chance of reaching a desirable angioplasty result, with less acute need for bailout stenting with higher procedure success.
CALCIUM 360 Trial economic analysis. The incremental cost of peripheral OA plus BA vs BA-only for critical limb ischemia was estimated using CALCIUM 360 trial data.23 Briefly, a deterministic simulation model used clinical and healthcare utilization data from the CALCIUM 360 trial and current cost data. Incremental cost of OA+BA vs BA-only included differential utilization during the procedure and adverse-event costs at 3, 6, and 12 months. For every 100 procedures, incremental annual costs to the hospital were US$350,930 lower with OA+BA compared with BA-only.23 In addition, in a probabilistic sensitivity analysis, cost savings were observed in 81.6% of the Monte Carlo simulations, indicating that OA+BA was a dominant treatment strategy.23 Despite higher upfront costs of OA, savings were realized due to reduced need for revascularization, amputation and end-of-life care over 6–12-month postoperative period. Thus, atherectomy with OA prior to BA was associated with cost savings to the hospital.23
COMPLIANCE 360 Trial. COMPLIANCE 360 was a prospective, multicenter, randomized controlled trial comparing acute and long-term outcomes of using OA and BA vs BA-only.24 Fifty patients presenting with Rutherford class 2-4 and femoropopliteal calcified lesions were randomized 1:1 into the two study arms: OA+BA vs BA-only. Balloon inflation pressure was significantly lower in the OA+BA group vs BA-only (4 vs 9.1 atm; P<.001), consistent with the findings in the CALCIUM 360 trial. All lesions in both cohorts were treated without adjunctive stenting as a standard unless to address a suboptimal result. Procedural success (residual stenosis < 30% without adjunctive stenting) occurred in 86.8% of lesions in the OA treatment group vs 18.5% in the BA-only group (P<.001). At 6 months freedom from TLR (including adjunctive stenting) or restenosis was significantly higher in the OA+BA group (77.1% vs 11.5%; P<.001).24 The authors of the CALCIUM 360 study concluded that compared to BA alone for the treatment of calcium-containing femoropopliteal lesions, OA pretreatment likely improves lesion compliance and leads to better luminal gain with lower balloon pressures, resulting in a marked reduction of adjunctive stenting.24 Patency at 12 months with OA therapy is similar to a provisional stent strategy despite minimal stent usage. Avoidance of in-stent restenosis and preserving future treatment options, by not placing a stent, are key advantages of the OA therapeutic approach.24
COMPLIANCE 360 Trial Economic Analysis. The clinical outcomes from the COMPLIANCE 360 trial (OA+BA vs BA-only for treatment of calcified femoropopliteal lesions) were correlated with cost data and previously published quality of life data.25 Site of service, hospital charges, and associated medical resource utilization were obtained from Uniform Billing statements for index treatments and associated revascularizations out to 1 year. Hospital costs were estimated using hospital-specific, procedure-specific cost-to-charge ratios. Length of stay and procedural data were collected from participating study sites. Twenty-five subjects with 38 lesions and 25 subjects with 27 lesions were randomized to the OA+BA and BA-only groups, respectively. Mean hospital charges (US$51,755 vs US$39,922) and estimated hospital costs (US$15,100 vs US$11,016) were numerically higher for OA+BA compared with BA-only. Stent utilization was significantly higher with BA-only treatment for all subjects (1.1 vs 0.1; P=.001) and in the subset of subjects with one lesion (1.0 vs 0.1; P<.001).25 There was a significant difference in cost for single-lesion vs multiple-lesion treatment. Using costs and quality-adjusted life years (QALYs) for the single-lesion cohort, the 1-year incremental cost of OA+BA vs BA-only was US$549, and incremental QALY was 0.16.25 This resulted in an incremental cost-effectiveness ratio of US$3,441, well below the US$50,000 threshold. One-year index procedure cost and cost-effectiveness were comparable for OA+BA vs BA only.25 This study provides compelling cost-effectiveness data for using atherectomy for treatment of calcified femoropopliteal lesions, a longstanding challenge for peripheral artery disease interventionalists.25
TRUTH study. The Tissue Removal Assessment with Ultrasound of the SFA and Popliteal (TRUTH) study assessed the performance of orbital atherectomy to treat femoropopliteal arteries, including determining its effect on plaque removal.26 Twenty-five patients with >70% stenosis in SFA, POP, or TPT arteries were enrolled at single center. Intravascular ultrasound (IVUS) images were collected pre- and post-OA and post-OA and BA. The mean maximum balloon inflation pressure was 5.2 ± 1.2 atm.26 Virtual histology IVUS (VH-IVUS) analysis revealed that at the maximum calcium ablation site calcium reduction was responsible for 86% of the lumen area increase.26 The minimum lumen area increased from 4.0 mm2 to 9.1 mm2 (P<.001), and the percentage of area stenosis decreased from 76.9% to 43.0% (P<.001) after OA+BA.26 At 12 months, the target-lesion revascularization rate was 8.2%, and ankle–brachial index and Rutherford classification improved significantly from baseline through follow-up. The authors concluded that the VH-IVUS analysis revealed that OA modifies the calcified component of the plaque burden. They further hypothesized that calcium modification by OA changes the lesion compliance, allowing for low pressure adjunctive BA.26
Lastly, a post hoc assessment of the TRUTH IVUS data was also completed to examine OA-mediated vessel wall injury. Briefly, the IVUS images were analyzed before and after OA for signs of a monolayer appearance of the arterial wall, which indicates disappearing medial and intimal layers and external elastic lamina.27 The analysis revealed that only 2 cases in the post-OA images indicated medial injury, suggesting that OA can treat calcific plaque while minimizing medial injury. The authors indicated that these promising results warrant additional studies to further understand the mechanism of action of OA and its impact on the medial layer of the vessel being treated. It was also concluded that the IVUS assessment methods described in the post hoc analysis may also be used by operating physicians to detect medial injury intraprocedurally and alter treatment strategy for possible adjunctive antirestenosis therapy with drug-eluting technologies.27
LIBERTY Trial. LIBERTY was a prospective, observational, core laboratory–assessed, multicenter trial of endovascular device intervention in 1204 subjects (mean age 69.8±10.7 years; 770 men) stratified by Rutherford category (RC): claudicants (RC2-3; n=501) and CLI with no/minimal tissue loss (RC4-5; n=603) or significant tissue loss (RC6; n=100).28,29 Key outcomes included quality of life (QoL) measures (VascuQol and EuroQol EQ-5D) and freedom from MAE, defined as death (within 30 days), major amputation, and target vessel revascularization (TVR) based on Kaplan-Meier (KM) analysis. The LIBERTY study design, endpoints, and data analysis plan were previously described in detail.29 Below we review some of the recently published LIBERTY results.
LIBERTY Trial 1-year results. Successful revascularization was beneficial, with RC improvement noted across all groups.28 Thirty-day freedom from MAE estimates were high across all groups: 99.2% in RC2-3, 96.1% in RC4-5, and 90.8% in RC6. At 12 months, freedom from MAE was 82.6% in RC2-3, 73.2% in RC4-5, and 59.3% in RC6 patients.28 Estimates for freedom from major amputation at 12 months were 99.3%, 96.0%, and 81.7%, respectively.28 QoL scores improved significantly across all domains in all groups with 12-month VascuQol total scores of 5.3, 5.0, and 4.8 for RC2-3, RC4-5, and RC6, respectively.28 The results indicate that peripheral endovascular intervention is a viable treatment option for RC2-3, RC4-5, and RC6 patients as evidenced by the high freedom from major amputation, as well as the improvement in QoL and the RC at 12 months. Furthermore, primary unplanned amputation is often not necessary in RC6.28
LIBERTY Trial 1-year CLI subanalysis. For this LIBERTY CLI subanalysis, RC5 and RC6 patients (RC5-6; N=404) were pooled and 1-year outcomes were assessed.30 Procedural complications rarely (1.7%) resulted in postprocedural hospitalization and 89.1% of RC5-6 patients were discharged to home. Considering the advanced disease state in RC5-6 patients, there was a high freedom from 1-year MAE rate of 65.5%.30 At 1 year, freedom from major amputation was 89.6%. Wounds identified at baseline on the target limb had completely healed in 172/243 (70.8%) of the RC5-6 subjects by 1 year. Additionally, the overall quality of life, as measured by VascuQoL, improved from baseline to 1 year.30 This analysis of LIBERTY RC5-6 patients demonstrates that peripheral endovascular device intervention can be successful in CLI patients, with low rates of major amputation and improvement in wound healing and QoL through 1-year follow-up.
LIBERTY Trial 3-year results. The 36-month KM survival rates were 86.0% in RC2-3, 79.8% in RC4-5, and 62.0% in RC6 groups.31 The KM estimates of freedom from major amputation at 36 months were 98.5% in RC2-3, 94.0% in RC4-5, and 79.9% in RC6. The 36-month KM estimates for freedom from TVR were 71.1% in RC2-3, 64.2% in RC4-5 and 61.9% in RC6 groups.31 Patients with claudication at baseline were at lower risk for MAEs compared with RC4-5 and RC6 patients during the 36-month follow-up. Vascular QoL improved from baseline and persisted up to 36 months in all patients.31 The results indicate that endovascular therapy is a viable treatment option for patients with symptomatic PAD, with sustained improved quality of life in both claudicants and patients with chronic limb-threatening ischemia through 3-years.31
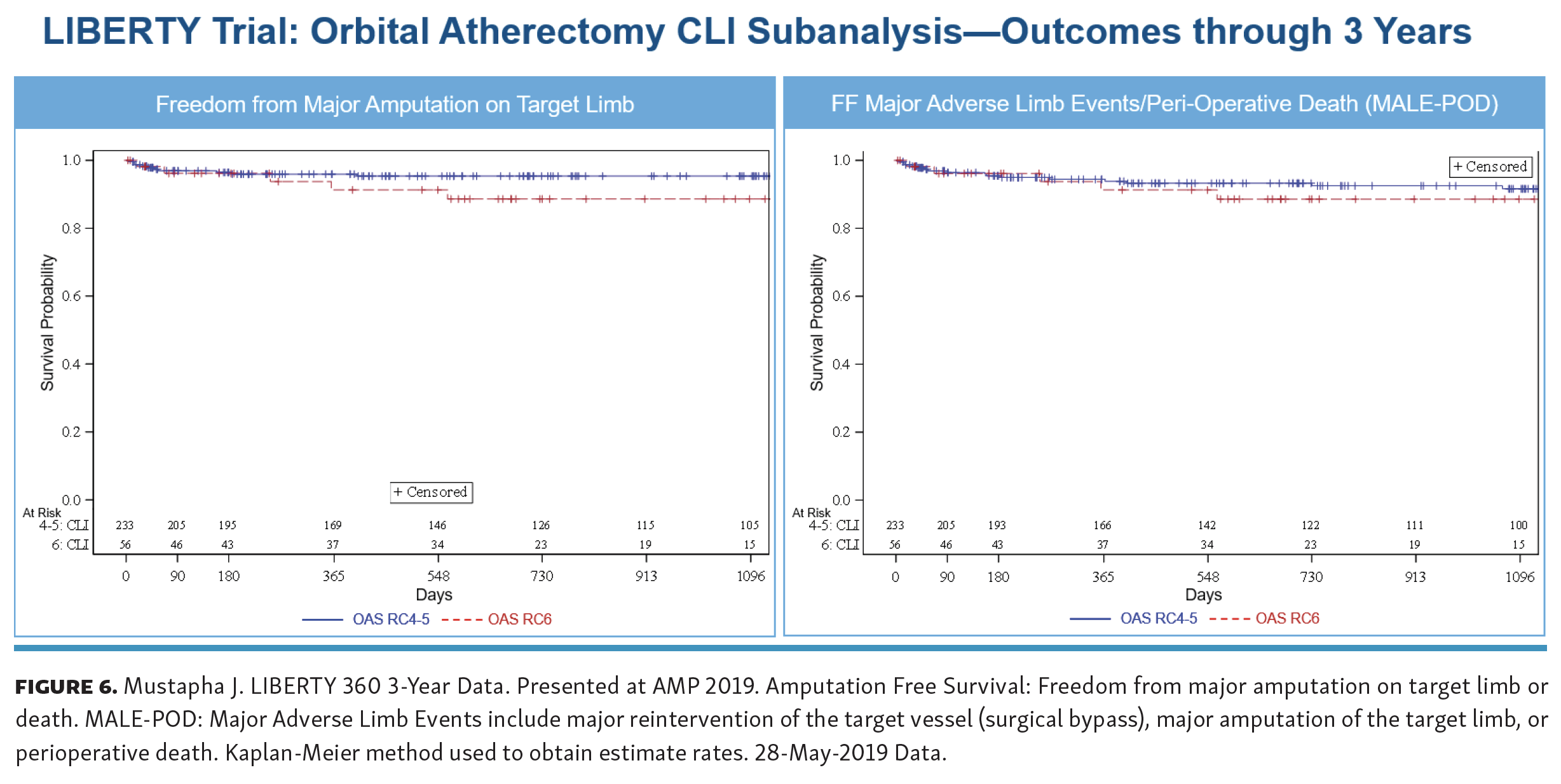
LIBERTY Trial 3-year orbital atherectomy subanalysis. Analysis of the LIBERTY trial identified 503 PAD patients with a total of 617 femoropopliteal and/or infrapopliteal lesions treated with any commercially available endovascular devices and adjunctive OA: RC2-3 (n=214), RC4-5 (n=233), or RC6 (n=56). The mean lesion lengths were 78.7 ± 73.7, 131.4 ± 119.0, and 95.2 ± 83.9 mm, respectively, for the 3 groups.32 After OA, balloon angioplasty was used in >98% of cases, with bailout stenting necessary in 2.0%, 2.8%, and 0% of the RC groups, respectively. A small proportion (10.8%) of patients developed angiographic complications, without differences based on presentation. During the 3-year follow-up, claudicants were at lower risk for MAE, death, and major amputation/death than patients with CLI. The 3-year KM survival estimates were 84.6% for the RC2-3 group, 76.2% for the RC4-5 group, and 63.7% for the RC6 group.32 The 3-year freedom from (FF) major amputation was estimated as 100%, 95.3%, and 88.6%, respectively.32Figure 6 shows the FF major amputation KM curve for the CLI subset. In addition, a contemporary endpoint of FF major adverse limb events-perioperative death (MALE-POD) is shown in Figure 6, indicating durable OA results from 1-year through 3-years in the CLI patient population (RC4-5: 94.4% to 91.6%, RC6: 91.3% to 88.6%).
{kind=link}
 Lastly, among CLI patients only, the RC at baseline was correlated with the combined outcome of major amputation/death, whereas RC classification did not affect TVR, MAE, major amputation, or death rates. The overall results indicate that peripheral artery angioplasty with adjunctive OA in patients with CLI or claudication is safe and associated with low major amputation rates after 3 years of follow-up.32 These results compare favorably with a Medicare claims data analysis of atherectomy which showed a 3-year mortality rate of 40.1% and amputation rate of 6.4% in the CLI patient population.33
Lastly, among CLI patients only, the RC at baseline was correlated with the combined outcome of major amputation/death, whereas RC classification did not affect TVR, MAE, major amputation, or death rates. The overall results indicate that peripheral artery angioplasty with adjunctive OA in patients with CLI or claudication is safe and associated with low major amputation rates after 3 years of follow-up.32 These results compare favorably with a Medicare claims data analysis of atherectomy which showed a 3-year mortality rate of 40.1% and amputation rate of 6.4% in the CLI patient population.33
Conclusions
The dual mechanism of peripheral orbital atherectomy (bi-directional differential orbital sanding and pulsatile forces) provides an effective and safe treatment of peripheral atherosclerotic lesions with varying levels of occlusion and calcification. The combination of plaque modification, improved vessel compliance, and lumen enlargement via OA can effectively restore blood flow in vessels above- and below-the-knee, relieving symptoms and improving limb salvage rates in patients with PAD and CLI. Numerous peripheral OA clinical trials have confirmed the high rates of procedural success, freedom from major adverse events, and freedom from amputation, as well as the economic value of orbital atherectomy.
Affiliations and Disclosures
From the 1Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, Michigan, Michigan State University College of Human Medicine, East Lansing, Michigan; 2Clinical Scientific Affairs, Cardiovascular Systems Inc., St. Paul, Minnesota; 3Division of Vascular Surgery, Baylor Medical Center, Houston, Texas; 4Vascular & Interventional Physicians, Gainesville, Florida; 5The Iowa Clinic, West Des Moines, Iowa; 6University of Southern California, California; 7Midwest Cardiovascular Research Foundation, Davenport, Iowa; 8North Carolina Heart and Vascular, Rex Hospital, UNC School of Medicine, Raleigh, North Carolina.
Advanced Cardiac & Vascular Centers for Amputation Prevention, Grand Rapids, MI and their affiliated university is Michigan State University College of Human Medicine, East Lansing, MI.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Mustapha reports consultant income from Cardiovascular Systems, Inc., Medtronic, Terumo, Philips, PQ Bypass, and BD Bard; stock options in CardioFlow. Dr Saab reports consultant income from Cardiovascular Systems, Inc., Medtronic, Terumo, Philips, PQ Bypass, BD Bard, and Gore; stock options in CardioFlow. Dr Adams reports consultant income, Data Safety Monitoring Board participation, and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events for Cardiovascular Systems, Inc. Dr Armstrong is a paid member of the Cardiovascular Systems, Inc. advisory board. Dr Shammas reports consultant income and educational grants from Cardiovascular Systems, Inc.; payment or honoraria for the speakers’ bureaus of Angiodynamics, Boston Scientific, BD, Janssen, Lilly, Esperion, and Boehringer. Dr Wiechmann reports consultant income from Boston Scientific, Philips, Veryan Medical, AngioDynamics, and BD; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events for Boston Scientific, Philips, Veryan Medical, AngioDynamics; and Data Safety Monitoring Board participation for Boston Scientific, Philips, Veryan Medical, AngioDynamics, MicroMedical Solutions. Dr Martinsen reports stock options and employment with Cardiovascular Systems, Inc. Ann Behrens reports stock options and employment with Cardiovascular Systems, Inc.The remaining authors report no conflicts of interest regarding the content herein.
Manuscript accepted May 24, 2021.
Address for correspondence: Jihad Mustapha, MD, Advanced Cardiac & Vascular Centers for Amputation Prevention, 1525 E. Beltline Ave, NE, Suite 101, Grand Rapids, MI 49503. Email: jmustapha@acvcenters.com